Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
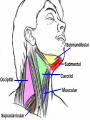
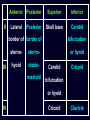
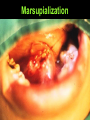
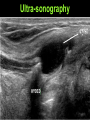
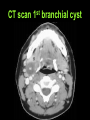
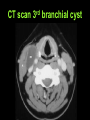
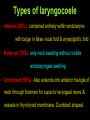
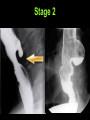
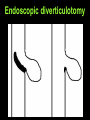
Neck Swellings Dr. Vishal Sharma Neck Triangles Anterior Triangle Boundaries: Anterior = midline of neck Posterior = S.C.M. anterior border Superior = lower border of mandible Floor = deep layer of deep cervical fascia Roof = Superficial layer of deep cervical fascia Subdivision: by digastric & omohyoid muscles into submental, submandibular, carotid, muscular Contents: carotid arteries, internal jugular vein, vagus, recurrent laryngeal nerves, submandibular gland, Levels I, II, III, IV & VI lymph nodes Posterior Triangle Boundaries: Posterior: Trapezius anterior border Anterior: S.C.M. posterior border Inferior: Middle 1/3rd of clavicle Floor: deep layer of deep cervical fascia Roof: Superficial layer of deep cervical fascia Subdivision: occipital & supra-clavicular by omohyoid Contents: subclavian artery, brachial plexus, spinal accessory nerve, level V lymph nodes Neck Lymph Nodes Sloan Kettering Classification Level I: Submental + submandibular nodes Level II: Upper jugular nodes (upper 1/3 of IJV) Level III: Middle jugular nodes (middle 1/3 of IJV) Level IV: Lower jugular nodes (lower 1/3 of IJV) Level V: Posterior triangle nodes Level VI: Anterior compartment nodes Level VII: Superior mediastinal nodes Submental Lymph nodes (Level Ia): Lateral: Anterior digastric belly (both sides) Inferior: Body of hyoid Submandibular Lymph nodes (Level Ib) Posterior: Posterior digastric belly Anterior: Anterior digastric belly Superior: Body of mandible Anterior Posterior II Lateral Posterior Superior Inferior Skull base Carotid border of border of III bifurcation sterno- sterno- or hyoid hyoid cleido- Carotid mastoid bifurcation Cricoid or hyoid IV Cricoid Clavicle Level V: Posterior triangle nodes Posterior: Trapezius anterior border Anterior: S.C.M. posterior border Inferior: Middle 1/3rd of clavicle Level VI: Anterior compartment nodes Superior: Body of hyoid bone Inferior: Supra-sternal notch Lateral: Lateral border of sterno-hyoid Level VII: Superior mediastinal nodes Classification of neck swelling according to position • Ubiquitous neck swellings • Midline neck swellings • Anterior triangle neck swellings • Posterior triangle neck swellings Ubiquitous neck swellings • Sebaceous cyst • Lipoma • Neurofibroma, schwannoma • Hemangioma • Dermoid cyst • Teratoma • Hydatid cyst Midline swellings Lymph node (submental, Delphian, suprasternal) Ludwig’s angina Sublingual dermoid Thyroglossal cyst Subhyoid bursitis Thyroid swelling (isthmus & pyramidal lobe) Laryngeal tumors Cold abscess Sternal tumor Thymus tumors Submandibular triangle swellings • Lymph node (level 1b) • Cold abscess • Submandibular salivary gland enlargement (deep lobe is bimanually ballotable) • Plunging ranula • Mandibular tumor Carotid + muscular triangle swellings Branchial cyst Branchiogenic cancer Laryngocoele (external) Thyroid lobe swelling Lymph node (II, III, IV) Cold abscess Carotid body tumour Carotid aneurysm Sternomastoid tumor of newborn Posterior triangle swellings Cystic hygroma Pharyngeal pouch (Zenker’s diverticulum) Lymph node (level V) Cold abscess Cervical rib Clavicular tumour Subclavian artery aneurysm Classification by etiology • Congenital / Developmental • Infectious / Inflammatory • Neoplastic: Benign / Malignant Congenital neck swellings a. Cystic Sebaceous cyst Dermoid cyst Branchial cyst Thyroglossal cyst Thymic cyst b. Solid: Ectopic thyroid c. Vascular Hemangioma Lymphangioma Inflammatory neck swellings • Lymphadenitis – Viral – Bacterial – Granulomatous • Sialadenitis – Parotid – Sub-mandibular • Deep neck space abscess Neoplastic neck swellings • Skin: Squamous cell Ca, Malignant melanoma • Soft tissue: – Benign: Lipoma, Fibroma, Schwannoma – Malignant: Rhabdomyosarcoma • Lymph node: Lymphoma, Metastasis • Thyroid: Benign / Malignancy • Vascular: Carotid body tumor, Angioma Hemangioma & lipoma Cervical Lymphadenopathy A. Inflammatory hyperplasia 1. Acute lymphadenitis 2. Chronic lymphadenitis 3. Granulomatous lymphadenitis Bacterial: tuberculosis, secondary syphilis Viral: infectious mononucleosis, AIDS Parasitological: toxoplasmosis Non-specific: sarcoidosis B. Neoplastic: lymphoma, lymphosarcoma, metastatic C. Lymphatic leukemia D. Autoimmune: systemic lupus erythematosus Lymph node consistency • Firm, rubbery: lymphoma • Soft : infection or cold abscess • Multiple, firm, shotty: syphilis, viral • Matted (connected): tuberculosis , sarcoidosis, malignant • Rock hard, immobile, fixed to skin: metastatic Tuberculous lymphadenitis • Involves upper deep cervical chain & posterior triangle lymph nodes • Development of peri-adenitis → matted nodes • Development of caseation → cold abscess • Abscess tracking down to skin forms subcutaneous collection → collar stud abscess • Abscess bursts spontaneously → tuberculous sinus Tuberculous lymphadenopathy Lymphoma More common in children & young adults 60 - 80% children with Hodgkin’s have neck mass Signs & symptoms: • Fever + malaise • Night sweats • Weight loss • Pruritus • Rubbery lymph nodes Metastatic lymph node • Seen in older patients • Level 1: oral cavity • Level 2, 3, 4: larynx, oropharynx, hypopharynx, thyroid • Level 5: nasopharynx • Left supraclavicular fossa: lung, stomach, testis Unknown Primary Lesion (UPL) Synonym: 1. metastasis of unknown origin 2. occult primary Definition: metastatic lymph node with primary site hidden or undetected Primary malignancy sites (as per frequency): 1. Nasopharynx 2. Oropharynx (base of tongue) 3. Hypopharynx (pyriform fossa) 4. Larynx 5. Thyroid Investigations for UPL 1. Fibreoptic nasopharyngoscopy + laryngoscopy 2. Rigid panendoscopy 3. Excision biopsy of I/L tonsil + blind biopsy of tongue base, pyriform fossa, fossa of Rosenmuller, tonsilo-lingual sulcus, retro molar trigone 4. CT scan from skull base to superior mediastinum 5. Excision biopsy of metastatic lymph node Ranula Introduction • Rana means frog (blue translucent swelling in floor of mouth looks like underbelly of frog) • Simple ranula: Bluish cyst located in floor of mouth. Painless mass, does not change in size in response to chewing, eating or swallowing • Plunging ranula: Sub-mandibular neck swelling with or without cyst in floor of mouth Simple Ranula Plunging ranula Plunging ranula Etiology • Simple ranula: partial obstruction or severance of sublingual duct leads to epithelial-lined retention cyst. Commonly traumatic. • Plunging ranula: 1. sublingual gland projects through or behind mylohyoid muscle 2. ectopic sublingual gland on cervical side of mylohyoid muscle Treatment Marsupialization: un-roofing of cyst & suturing of cyst margin to adjacent tissue. Failure = 60-90% Sclerosing agents: intra-lesional injection of Bleomycin or OK-432 Intra-oral excision: of ranula alone (failure = 60%) or ranula + sublingual gland (failure = 2 %) Trans-cervical approach for plunging ranula: complete removal of cyst + sublingual gland Marsupialization Intra-oral excision Ranula specimen Thyroglossal cyst Embryology • Thyroid appears as epithelial proliferation in floor of mouth. Thyroid descends in front of pharynx as bi-lobed diverticulum, connected to tongue by thyroglossal duct. • The duct normally disappears later. Thyroglossal cysts are cystic remnant of thyroglossal duct. • Commonest congenital anomaly of thyroid Location • Cyst may lie at any point along migratory pathway of thyroid gland • Commonest site: sub-hyoid (50%) • Second common site: supra-hyoid . • Other common sites: base of tongue, at level of thyroid cartilage, sublingual • Least common site: at level of cricoid cartilage Location 1 = base of tongue 2 = sublingual 3 = supra-hyoid 4 = sub-hyoid 5 = in front of thyroid cartilage 6 = in front of cricoid cartilage Clinical features • Commonly seen in early childhood • Midline, round swelling, 2-4 cm in diameter • Swelling moves up with swallowing • Swelling moves up with protrusion of tongue • Swelling mobile horizontally but not vertically • Cyst increases in size with URTI Neck swelling moving with swallowing • Thyroid swelling • Thyroglossal cyst (mobile horizontally) • Subhyoid bursitis (oval, long axis horizontal) • Pre-laryngeal & pre-tracheal lymph nodes • Laryngocele Midline neck swelling Ultra-sonography CT scan axial cut MRI sagittal cut Sistrunk’s operation Consists of complete surgical excision of cyst & its tract along with body of hyoid bone & core of tongue tissue around suprahyoid tongue base up to foramen caecum Thyroid scan mandatory before cyst excision as cyst may contain only functioning thyroid tissue Patient position & incision Exposure of cyst + tract Exposure & cutting of hyoid bone Removal of tongue tissue Removal of cyst + tract Complications 1. Infection of cyst & abscess formation 2. Throglossal fistula 3. Malignancy (1%) Infected cyst Thyroglossal fistula Branchial cleft cysts Embryology Branchial anomalies • Cyst: remnant of branchial clefts or pouch without internal or external opening • Sinus: persistence of cleft with skin opening • Fistula: persistence of both cleft + pouch with openings in skin & pharynx • Fistula tract lies caudal to structures derived from its arch & dorsal to structures of following arch Branchial anomalies • In children, fistulas are more common than sinuses, which are more common than cysts • In adults, cysts predominate • Branchial cleft anomalies + biliary atresia + congenital cardiac anomalies = Goldenhar's complex First branchial cleft cyst • Type I: Contains only ectodermal elements without cartilage or adnexal structures. Present as duplication of external auditory canal. • Type II: Contains both ectoderm & mesoderm. Present as abscess below angle of mandible. • Fistula ends internally around Eustachian tube Second branchial cleft cyst • Commonest branchial anomaly • Painless, fluctuant mass along anterior border of middle 1/3rd of sternocleidomastoid muscle • Fistula tract opens externally along lower 1/3rd of SCM, passes deep to 2nd arch structures (external carotid, stylohyoid muscle, posterior belly of digastric); superficial to internal carotid (3rd arch); ends internally in tonsillar fossa Second branchial cleft cyst Second branchial cleft cyst Third branchial cleft cyst • Painless, fluctuant mass along anterior border of lower 1/3rd of sternocleidomastoid muscle • Fistula tract opens externally along lower 1/3rd of SCM, passes deep to 3rd arch structures (internal carotid, glossopharyngeal nerve); superficial to superior laryngeal nerve (4th arch): opening internally in base of pyriform fossa Fourth branchial cleft cyst • Presents as mass along anterior border of lower 1/3rd of stenomastoid or as recurrent thyroiditis • Fistula tract opens externally along lower 1/3rd of SCM, passes deep to 4th arch structures (superior laryngeal nerve ); superficial to recurrent laryngeal nerve (6th arch); opening internally in apex of pyriform fossa CT scan st 1 branchial cyst CT scan nd 2 branchial cyst CT scan rd 3 branchial cyst Coronal MRI Sagittal MRI Axial MRI Treatment • Abscesses treated first with incision & drainage + broad-spectrum antibiotics • Elective surgical excision of cyst with its tract traced up to its origin in pharyngeal wall done after infection resolves • Branchial fistula excised with 2 horizontally placed incisions (stepladder incision) Excision of branchial cyst Branchial fistula excision Laryngocoele • Arises from expansion of saccule of laryngeal ventricle due to ed intra-luminal pressure in larynx or congenital large saccule Causes of ed intra-luminal pressure in larynx: • Occupational (?): trumpet players, glass blowers • Coexistence of larynx cancer • Male : female 5:1, Peak age = 6th decade, Unilateral in 85 % cases, 1% contain carcinoma Swelling enlarges on Valsalva Types of laryngocoele • Internal (20%): contained entirely within endolarynx with bulge in false vocal fold & aryepiglottic fold • External (30%): only neck swelling without visible endolaryngeal swelling • Combined (50%): Also extends into anterior triangle of neck through foramen for superior laryngeal nerve & vessels in thyrohyoid membrane. Dumbbell shaped. Types of laryngocoele Internal External Combined 89 Clinical Features • Hoarseness • Stridor in large endolaryngeal laryngocoele • Neck swelling • Manual compression of neck swelling results in escape of fluid / gas into airway (Boyce’s sign) • 10% cases are pyocele: sore throat, cough Flexible laryngoscopy ▪ Swelling of false vocal folds & ary-epiglottic fold ▪ Swelling easily emptied ▪ Escape of purulent fluid into airway = pyocoele 91 X-ray neck AP view X-ray soft tissue neck AP view during Valsalva maneuver shows airfilled radiolucent swelling 92 CT scan: mixed laryngocoele Treatment • No symptom: no treatment • Infected laryngocoele: aspiration & antibiotics • Internal laryngocoele: endoscopic marsupialization • External laryngocoele: Excision by external approach. Cyst exposed by removing upper half of thyroid cartilage. Cyst incised at its neck & stitched. Endoscopic marsupialization External approach Carotid body tumor • Pulsating, compressible mass in carotid triangle • Mobile only horizontally not vertically • Angiography: vascular mass b/w external & internal carotid arteries (Lyre’s sign) • Rx: Radiation or close observation in elderly. Surgical resection for small tumors in young patients with hypotensive anesthesia & preoperative measurement of catecholamines. Lyre sign Sternomastoid tumor of infancy • Firm mass of SCM, becomes prominent when chin turned away & head tilted towards the mass • Due to birth trauma causing infarction / hematoma with subsequent fibrotic replacement • Rx: Physical therapy. Myoplasty of SCM for refractory cases. Hypopharyngeal pouch Introduction • Hypopharyngeal pouch is an acquired pulsion diverticulum caused by posterior protrusion of mucosa through pre-existing weakness in muscle layers of pharynx or esophagus • In contrast, congenital diverticulum like Meckel's diverticulum is covered by all muscle layers of visceral wall Weak spots b/w muscles Origin of Zenker’s diverticulum Etiology 1. Tonic spasm of cricopharyngeal sphincter: C.N.S. injury Gastro-esophageal reflux 2. Lack of inhibition of cricopharyngeal sphincter 3. Neuromuscular in-coordination between thyropharyngeus & cricopharyngeus 4. Second swallow against closed cricopharynx These lead to increased intra-luminal pressure in hypopharynx & mucosa bulges out via weak areas Clinical features 1. Entrapment of food in pouch: sensation of food sticking in throat & later dysphagia 2. Regurgitation of entrapped food: leads to foul taste bad odor nocturnal coughing choking 3. Hoarseness: due to spillage laryngitis or sac pressure on recurrent laryngeal nerve 4. Weight loss: due to malnutrition 5. Compressible neck swelling on left side: reduces with a gurgling sound (Boyce sign) Complications 1. Lung aspiration of sac contents 2. Bleeding from sac mucosa 3. Absolute oesophageal obstruction 4. Fistula formation into: trachea major blood vessel 5. Squamous cell carcinoma within Zenker diverticulum (0.3% cases) Investigations • Chest X-ray: may show sac + air - fluid level • Barium swallow • Barium swallow with video-fluoroscopy • Rigid Oesophagoscopy • Flexible Endoscopic Evaluation of Swallowing Barium swallow Barium swallow with Video-fluoroscopy Rigid Esophagoscopy Staging Lahey system: • Stage I: Small mucosal protrusion • Stage II: Definite sac present, but hypo-pharynx & esophagus are in line • Stage III: Hypopharynx is in line with pouch & esophagus pushed anteriorly Stage 1 Stage 2 Stage 3 Surgical Treatment 1. Cricopharyngeal myotomy: combined with others 2. Diverticulum invagination: Keyart 3. Diverticulopexy: Sippy-Bevan 4. External or open Diverticulectomy: Wheeler 5. Rigid Endoscopic Diverticulotomy Cautery (Dohlman) Laser Stapler 6. Flexible Endoscopic Diverticulotomy with Laser Treatment Protocol 1. Small sac (< 2cm): Cricopharyngeal (CP) myotomy + invagination 2. Large sac (2-6 cm): Open Diverticulectomy with CP myotomy or Endoscopic Diverticulotomy with CP myotomy 3. Very large sac (> 6 cm): Open Diverticulectomy with CP myotomy or Diverticulopexy with CP myotomy Cricopharyngeal myotomy Diverticulum invagination Diverticulum pushed into hypopharynx lumen & muscle + adjacent tissue are oversewn. CP myotomy is usually combined with this. External diverticulectomy Endoscopic diverticulotomy Diverticuloscope advanced so its upper lip is within esophagus & lower lip is within diverticulum View through diverticuloscope Cautery, laser, or stapling device used to divide common party wall between pouch & esophagus View through diverticuloscope Endoscopic diverticulotomy Dohlman’s instruments Diverticulopexy Sac mobilized & its fundus fixed to sternocleidomastoid muscle in a superior, non-dependent position. CP myotomy is also done. Cystic hygroma • Synonym: cystic lymphangioma • Definition: congenital, benign, multi-loculated, lymphatic lesion classically found in posterior triangle of neck • Other sites: axilla, mediastinum, groin & retroperitoneum • Etiology: failure of lymphatics to connect to venous system; abnormal budding of lymphatic tissue; sequestered lymphatic cell rests Clinical Features • 50-65% cases present at birth, 80-90% by 2 years • Soft, painless, compressible trans-illuminant mass present in posterior triangle of neck. Overlying skin can be bluish or normal . Sudden se in size due to infection or intra-cystic bleeding. • Look for tracheal deviation, airway obstruction, cyanosis, feeding difficulty, failure to thrive Stage Clinical Features Complication rate Stage I U/L infrahyoid 20% Stage II U/L suprahyoid 40% Stage III U/L infrahyoid + suprahyoid 70% Stage IV B/L suprahyoid 80% Stage V B/L infrahyoid + suprahyoid 100% Cystic hygroma Investigations • USG: used to detect CH in utero • CT scan: Contrast helps to enhance cyst wall visualization & relationship to surrounding blood vessels. CH appears isodense to CSF. – Macrocystic: cystic spaces > 2 cm – Microcystic: cystic spaces < 2 cm • MRI: Best investigation. CH appears hyperintense on T2 & hypointense on T1-weighted images. MRI: CH causing airway compression Treatment • Asymptomatic: 1. watchful waiting 2. sclerosing agents: OK-432 (Picibanil), bleomycin, ethanol, doxycycline, Interferon, fibrin sealant • Infected cases: intravenous antibiotics & drainage; definitive surgery after 3 months • Surgical excision: mainstay of treatment. Done with Cautery, Laser, Radiofrequency • Acute stridor: aspiration, emergency tracheostomy Kawasaki syndrome • Etiology: idiopathic multisystem vasculitis • Diagnosis (presence of any 5): 1. Fever > 5 days. 2. Conjunctival injection. 3. Red / desquamated palm / sole. 4. Injected oral cavity 5. Polymorphous rash. 6. Cervical lymph node enlargement • Permanent cardiac damage in 20% untreated cases • Rx: high dose aspirin & immunoglobulin Thank You 135