Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
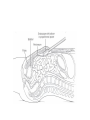
INGUINAL HERNIA REPAIR: OPEN vs TEP APPROACHES Prof Dr Orhan Alimoğlu Department of General Surgery Istanbul Medeniyet University Inguinal hernia • One of the most common surgical problem in daily practice • Different operations and approaches • Gold standard: repair with mesh • Currently – Lichtenstein hernia repair – Endoscopic totally extra-peritoneal (TEP) repair – Laparoscopic trans-abdominal preperitoneal (TAPP) repair General Precautions • No place for routine antibiotic and thromboembolic prophylaxis, only in selected patients • Risk factors for wound and mesh infection – – – – – – Advanced age Corticosteroid use Immunosuppression Obesity Diabetes Malignancy Characteristics of mesh • • • • Large vs small Low-weight vs heavy weight Micropore vs macropore Conclusion: Efficiency of lighter mesh with larger pores only during the first few postoperative weeks Lichtenstein Inguinal Hernia Repair • Large mesh (7*15 cm) – 2 cm medial to the pubic tubercle, 3–4 cm above the Hesselbach’s triangle, and 5–6 cm lateral to the internal ring, trimming 3–4 cm from its lateral side • Crossing and suturing tails of mesh behind spermatic cord • Securing mesh with two interrupted sutures on upper edge and one continuous suture with no more than three to four passes on lower edge of mesh • Keeping mesh with a slightly relaxed, tented up, or dome-shaped configuration • Identification and protection of the ilioinguinal, iliohypogastric, and genital nerves Advantages • • • • • Every type of inguinal hernia Local anesthesia Easy to learn and perform Low rate of recurrence Gold standard? Disadvantages • Postoperative chronic pain – Higher than TEP or TAPP ? • Return to daily activity – Later than TEP or TAPP ? TEP Inguinal Hernia Repair • Technique – Trocars • Direct access of one subumblical 10 mm and two 5 mm at the midline – Preperitoneal dissection – Dissection of hernial sac – Parietalization of spermatic cord and its content – Placement of mesh Technical difficulties • Preperitoneal space creation – Baloon dissection in early learning curve besides its cost • Peritoneal injury – Loss of exposure – Closure of defect via pretied suture, loop ligation, endoscopic stapling or endoscopic suturing • Port-site closure – Closure of fascial defects larger than 10 mm Dissection and Landmarks • Superior • Pubic bone – Subumblical area • Cooper’s ligament • Inferior • Inferior epigastric – Space of Retzius vessels • Inferolateral • Cord structures – Psoas muscle and Bogros • Myopectineal orifice space boundaries • Medial • Fascia over psoas – Beyond midline muscle Controversies • Preoperative urinary catheterization – Preoperative emptying of urinary bladder by him/herself – Catheterization in difficult and long-standing surgery • Access for pneumopreperitoneum – Subumblical direct trocar vs suprapubic Veress Technical Key Points • Inversion and anchoring of direct sac to Cooper’s ligament to decrease risk of seroma and hematoma formation • Proximal ligation and distal division of large indirect hernia sac • Drains only in selected patients • Fixation of mesh in hernias greater than 4 cm Recommendations • Larger mesh (12*17 cm) in larger hernia (>3-4 cm) • Stapled fixation of mesh to the symphysis, Cooper’s ligament and rectus muscle in larger direct hernia (>3-4 cm) • Overlapping of mesh approximately 1-3 cm lateral to the spina iliaca anterior superior in large indirect hernias (>4-5) Advantages of TEP repair • Early return to daily activities • Low rate of postoperative chronic pain • Exploration of contralateral side for hidden hernias ? Disadvantages of TEP repair • General anesthesia; regional anesthesia in selected patients • Longer learning curve – At least 50 to 60 cases • Applicability on incarcerated and scrotal hernias • Applicability on patients with previous lower abdominal surgery Learning Curve for TEP repair • Can J Surg, 2012, 55: 33-6 – 700 patients – Learning curve after the first 60 cases • A plateau of less than 30 min for duration of surgery • A plateau of 1 day for length of stay • Conclusion: learning curve for TEP hernia repair as 60 cases for a beginner surgeon