Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
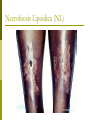
Cutaneous Manifestations of Internal Disease Residents’ Conference Hallie McDonald, MD August 16, 2005 Diabetes Mellitus According to Perez et al (3) ,approximately 30% of patients with DM develop skin lesions at some point Overall prevalence of cutaneous disorders does not differ between type I and type II diabetics Type I patients get more autoimmune-type lesions Type II patients get more cutaneous infections Diabetes Mellitus Cutaneous lesions usually appear after the development of DM, but may be the first presenting sign Four major groups of skin findings 1. 2. 3. 4. Skin diseases associated with DM (necrobiosis lipoidica and diabetic bullae) Cutaneous infections Cutaneous manifestions of diabetic complications (neuropathic ulcers) Skin reactions to diabetic treatment Necrobiosis Lipoidica (NL) NL appears in 0.3-1.6% of diabetics (2,4) Anywhere from 11-65% of patients with NL have DM at the time of skin dx (2,7,8) If they do not have DM at time of dx, about 90% will develop diabetes, have abnormal glucose tolerance, or report parents with DM (2, 4) Diabetic control has no effect on the course of NL. Necrobiosis Lipoidica (NL) NL is 3x more common in women. According to Jelinek, (9) NL appears earlier (mean age 22) in Type I diabetics than Type II (mean age 49.) Appearance Begins as an oval, violaceous patch and expands slowly. Advancing border is red. Central area turns yellowish brown. Central area atrophies and telangiectasia become evident. 13% of cases progress to ulceration Necrobiosis Lipoidica (NL) Classically, NL occurs bilaterally on the pretibial or medial malleolar areas. Not painful. Spontaneous resolution occurs in 13-19% with residual scarring. Treatment: potent topical steroids, intralesional steroids at the active border, or rarely systemic steroids Necrobiosis Lipoidica (NL) Necrobiosis Lipoidica (NL) Necrobiosis Lipoidica (NL) Necrobiosis Lipoidica (NL) Necrobiosis Lipoidica (NL) Granuloma Annulare (GA) Controversy surrounds the association between GA and DM. A case-control study by Nebesio et al. (5) failed to reveal a statistically significant correlation between the two. A retrospective study by Studer et al. (6) suggested that up to 12% of patients presenting with GA had DM. Despite conflicting studies, it is reasonable to screen patients presenting with GA for DM. Granuloma Annulare (GA) Appearance Histology Ring of small, firm, flesh-colored or red papules If localized, most frequently found on lateral and dorsal surfaces of hands and feet Disease begins with an asymptomatic, flesh-colored papule that undergoes central involution Over months, a ring of papules grows Can spontaneously regress without scarring Focal degeneration of collagen in the upper and middermis, palisaded histiocytes around collagen bundles, and abundant dermal mucin Pathogenesis unknown Granuloma Annulare (GA) Treatment If localized, best left untreated. Can treat with intralesional steroids, if needed If generalized, can also use dapsone, isotretinoin, freezing, cyclosporin, or PUVA. Granuloma Annulare (GA) Granuloma Annulare (GA) Granuloma Annulare (GA) Granuloma Annulare (GA) Granuloma Annulare (GA) Granuloma Annulare (GA) Granuloma Annulare (GA) Histology showing focal degeneration of collagen in the upper and mid-dermis, palisaded histiocytes around collagen bundles, and abundant dermal mucin Diabetic Bullae Approximately 0.5% of diabetics (2) More common in men with long-standing DM and neuropathy Two types have been described Pathogenesis not well-understood More frequent, non-scarring lesions with a histologic intraepidermal split without acantholysis Less common, occasionally hemorrhagic bullae that heal with scarring, slight atrophy, and have a histologic subepidermal split Could be related to trauma with reduced threshold for blister formation Other theories include immunologic factors, disturbed catabolism of calcium, magnesium, or carbohydrates, microangiopathy, and vascular insufficiency Appearance Painless bullae on non-inflamed base that appear suddenly Most common on the dorsa and sides of lower legs and feet, sometimes with similar lesions on the hands and forearms Bullae contain clear, sterile fluid Diabetic Bullae Bullae tend to heal spontaneously in 2-5 weeks Bullosis diabeticorum remains a diagnosis of exclusion with negative immunofluorescence studies, porphyrin levels, and cultures DDx: bullous pemphigoid, epidermolysis bullosa acquisita, porphyria cutanea tarda, bullous impetigo, erythema multiforme, and coma blisters May recur in the same or new locations If large and symptomatic, can aspirate the fluid leaving an intact blister roof as a wound covering Diabetic Bullae Diabetic Bullae Diabetic Bullae Histology showing a noninflammatory blister with a subepidermal and focally intraepidermal separation Acanthosis Nigricans Seen in situations of insulin resistance Besides in DM, also seen in the following: Carcinomas, especially of the stomach Secondary to meds (nicotinic acid, estrogen, or corticosteroids) Pineal tumors Other endocrine syndromes (PCOS, acromegaly, Cushing’s disease, hypothyroidism) Obesity Pathogenesis According to Cruz (12) , it may be related to insulin binding insulin-like growth factor receptors on keratinocytes and dermal fibroblasts, thus stimulating growth. Acanthosis Nigricans Appearance Hyperpigmented, velvety plaques in body folds, mostly axillae and neck Can also present on groin, umbilicus, areolae, submammary areas, and on the hands (tripe hands) Treatment- usually asymptomatic Weight loss Retinoic acid and salicylic acid Acanthosis Nigricans Acanthosis Nigricans Acanthosis Nigricans Skin Infections in DM Occur in 20-50% of poorly controlled diabetics (2, 4) More common in Type II May be related to abnormal microcirculation, hypohidrosis, PVD, neuropathy, decreased phagocytosis and killing activity, impaired leukocyte adherence, and delayed chemotaxis all seen in diabetics (2, 9, 10, 11) Skin Infections in DM Fungal infections- most common Candida Candidal paronychia Inframammary candida Genital candida Psedudohyphae and spores on KOH prep support dx of Candida Purulent drainage may indicate secondary bacterial infection Because maceration and skin breaks can serve as portals of infection, tinea pedis should be treated aggressively in diabetics Treatment includes drainage of any abscesses, keeping the digits dry, and topical antifungals (clotrimazole) Candidiasis in Diabetics White, curdlike material adherent to erythematous, fissured oral commisure; angular stomatitis Candidiasis in Diabetics Initial pustules on erythematous base that become eroded and confluent Candidiasis in Diabetics Candidiasis in Diabetics Candidiasis in Diabetics Candidiasis in Diabetics KOH prep showing pseudohyphae and budding yeast forms Skin Infections in DM Bacterial Infections- can be more severe and widespread in diabetics Malignant otitis externa Pseudomonas aeruginosa Fatal in over 50% patients (13) Can progress to chondritis, osteomyelitis, and bacterial meningitis Treat up to 3 months with oral quinolones but may need IV antibiotics Malignant Otitis Externa in Diabetics Skin Infections in DM Bacterial infections in DM Erythrasma Reddish tan scaling patches of the upper inner thighs, axillae, toe web spaces, and inframammary creases Gram positive Corynebacterium minutissimum Identified with Wood’s light coral fluorescence Treat with oral erythromycin for 5 days Erythrasma in Diabetics Reddish tan scaling patches of the upper inner thighs, axillae, toe web spaces, and inframammary creases Erythrasma in Diabetics Erythrasma in Diabetics Wood’s Lamp in the Diagnosis of Erythrasma Cutaneous Manifestations of Diabetic Complications: Foot Ulcers Responsible for 70% of annual lower limb amputations in the U.S.(2) Large economic impact from medical and surgical therapy, rehab, loss of work, and mortality Prevention is key Daily foot inspections, appropriate footwear Causes for ulcer formation: Peripheral neuropathy (60-70%) Vascular disease (15-20%) Treatment: aggressive debridement and offloading or with a contact cast Treatment: surgical re-vascularization Combination of peripheral neuropathy and vascular disease (15-20%) Cutaneous Reactions to Diabetic Treatment Insulin Allergy may be local or systemic and usually occurs within the first month of therapy Lipoatrophy can also occur Erythematous or urticarial pruritic nodules at the site of injection Circumscribed depressed areas of skin at the insulin injection site 6-24 months after starting insulin More common in women and children Pathogenesis unknown but may be related to lipolytic components of the insulin preparation, an immune complex-mediated inflammatory process with lysosomal enzyme release, cryotrauma from refrigerated insulin, or mechanical trauma from injection Lipohypertrophy can also occur Soft dermal nodules that resemble lipomas at sites of frequent injection May be a response to the lipogenic action of insulin Treat and prevent by rotating sites of injection Cutaneous Reactions to Diabetic Treatment: Lipoatrophy Cutaneous Reactions to Diabetic Treatment- Insulin Highly purified or recombinant insulins have a reduced allergy prevalence (0.1-0.2%) (4) Observe the patient’s technique to make sure it isn’t intradermal Treatment includes substitution of a more purified insulin, discontinuation or desensitization for severe systemic rxns Cutaneous Reactions to Diabetic Treatment-Oral Hypoglycemics Most rxns are associated with the first-generation sulfonylureas (chlorpropamide and tolbutamide) 1-5% of patients on these drugs will develop skin rxns during the first 2 months of treatment (2,4) Most commonly, they present with maculopapular eruptions that resolve despite continuation of the drug For patients of chlorpropamide, 10-30% will develop a disulfiram-like rxn of flushing, headache, tachycardia, and shortness of break after ingesting alcohol. This seems to be autosomal dominant. (2,3) Second-generation sulfonylureas can also be associated with cutaneous rxns. Hyperthyroidism and the Skin Thyroid hormone plays a pivotal role in the growth and formation of hair and sebum production. Thyroid hormone stimulates epidermal oxygen consumption, protein synthesis, mitosis, and determination of epidermal thickness. There is increased cutaneous blood flow and peripheral vasodilation. Hyperthyroidism and the Skin Skin is usually warm, moist, and smooth Facial flushing Palmar erythema Hyperpigmentation, esp. creases of palms and soles, gingiva, and buccal mucosa Hyperhydrosis, particularly of palms and soles Scalp hair can be soft, fine and sometimes accompanied by non-scarring alopecia 5% of patients with hyperthyroidism have nail findings (14) Plummer’s Nail in Hyperthyroidism “Plummer’s nail”: concave contour and distal onycholysis, esp. the ring finger (not specific- also seen in hypothyroidism, psoriasis, after trauma, or in allergic contact dermatitis) Scleromyxedema in Hyperthyroidism Numerous firm white, yellow, or pink papules on face, trunk, axillae, and extremities Lesions result from accumulation of hyaluronic acid in the dermis, accompanied by large fibrocytes (14, 15) Can be accompanied by weight loss, esophageal dysmotility, vascular dz, Raynaud’s phenomenon, monoclonal gammopathy, neurologic manifestations, joint dz, and myopathy (14) Treatment of hyperthyroid state with radioactive iodine does not improve skin findings (14, 16) Scleromyxedema in Hyperthyroidism Firm white, yellow, or pink papules on face, trunk, axillae, and extremities Scleromyxedema in Hyperthyroidism Graves’ Disease These patients can have all of the other previously mentioned cutaneous manifestations of hyperthyroidism in addition to several unique entities Pretibial myxedema (0.5-4% of patients) Presentation varies from “peau d’orange” appearance to extensive infiltration that mimics elephantitis vurrucosa nostra Most often, bilateral, asymmetric, raised, firm plaques or nodules varying from pink to brown, sometimes with woody induration Can appear anywhere (arms, shoulders, head) Can treat with topical steroids, intralesional steroids, IV pulse steroids, or IVIG Pathogenesis remains unknown, but one theory suggests pretibial fibroblasts are the target for antithyroid antibodies(14) In support of this theory, Wu et al. (16) reported the presence of TSH and TSH receptor antibody binding in fibroblasts as well as the presence of RNA encoding the extracellular domain of the TSH receptor. Pretibial Myxedema in Graves’ Disease Bilateral, asymmetric, raised, firm plaques or nodules varying from pink to brown, sometimes with woody induration Pretibial Myxedema in Graves’ Disease Pretibial Myxedema in Graves’ Disease Thyroid Acropachy in Graves’ Disease Thyroid acropachy (1% of Graves’ patients) Triad of digital clubbing, soft tissue swelling of hands and feet, and periosteal new bone formation Graves’ Disease and Thyroid Acropachy AP radiograph of the hand demonstrates feathery periosteal bone proliferation of the diaphyses of the metacarpals and proximal phalanges Hypothyroidism and the Skin Skin changes in hypothyroidism reflect a hypometabolic state and subsequent reduced core body temperature results in cutaneous vasoconstriction. (14) Skin is cool, dry, and pale. Pallor results from cutaneous vasoconstriction and increased deposition of water and mucopolysaccharides in the dermis, which alter the refraction of light Hypohydrosis may lead to palmoplantar keratoderma Carotenemia (from decreased hepatic conversion of beta carotene to Vit A) gives skin yellowish hue (14, 17) Hair: dry, brittle, coarse; partial alopecia Loss of hair from lateral 1/3 of eyebrows Hypothyroidism Facies with Generalized Myxedema Generalized myxedema Occurs as a result of deposition of dermal acid mucopolysaccharides (esp. hyaluronic acid and chondroitin sulfate) in the skin Skin is non-pitting Face: swollen lips, broad nose, macroglossia, and puffy eyelids Thyroid Disease and Other Cutaneous Disease Associations Autoimmune thyroid disease has been associated with other cutaneous diseases Alopecia areata (18) Bullous disorders Vitiligo Pemphigus foliaceus Pemphigus vulgaris (19) (20) Derived from the Greek vitelius, signifying a “calf's white patches” Fairly symmetric pattern of white macules with welldefined borders Connective tissue diseases Dermatomyositis (21) , SLE (22) , scleroderma(23) Alopecia Areata Associated with Autoimmune Thyroid Disease Rapid onset of total hair loss in a sharply defined, usually round, area Regrowth begins in 1 to 3 months and may be followed by loss in the same or other areas Pemphigus foliaceus Associated with Autoimmune Thyroid Disease Pemphigus foliaceus: recurrent shallow erosions, erythema, scaling, and crusting Pemphigus vulgaris Associated with Autoimmune Thyroid Disease Painful oral erosions usually precede the onset of skin blisters by weeks or months Pemphigus vulgaris Associated with Autoimmune Thyroid Disease Nonpruritic flaccid blisters varying in size from 1 to several cm appear gradually on normal or erythematous skin Invariably generalize if left untreated Cutaneous Paraneoplastic Syndromes In 1976, Helen Ollendorff Curth set criteria that should be met before a skin disease can be called a paraneoplastic dermatosis (24,25) : Both conditions start approximately the same time Both conditions follow a parallel course Neither the onset nor the course of either condition is dependent on the other A specific tumor occurs with a specific skin manifestation The dermatosis is not common in the general population A high percentage of association between the two conditions is noted Currently, only the first two criteria should be met to call a skin disease a paraneoplastic process (24, 25) . Cutaneous Paraneoplastic Syndromes May be initial clue to underlying neoplasm Can herald the recurrence of a malignancy Examples Necrolytic migratory erythema Sign of Leser-Trelat Hypertichosis lanuginosa acquisita Bazex’s syndrome Dermatomyositis Erythroderma Necrolytic Migratory Erythema Glucagonoma syndrome includes glucose intolerance, weight loss, anemia, hair and nail changes, hypoaminoaciduria, psychiatric disturbances, and thromboembolic disease (24, 26) Skin manifestation of the glucagonoma syndrome Pathophysiology is not known, but it is probably related to catabolism from increased levels of glucagon When physician suspects this, be aggressive Erythematous macules and papules, often annular or arciform, on central face, lower abdomen, perineum, groin, buttocks, and thighs Progress to erosions secondary to epidermal necrosis Skin disease has waxing and waning course that does not seem to follow the course of the glucagonoma 75% glucagonomas are metastatic at time of diagnosis(27) Gold standard for treatment is surgery Necrolytic migratory erythema Erythematous macules and papules, often annular or arciform than can progress to erosions Sign of Leser-Trelat First described in 1890 as an increase in the number of cherry angiomas in patients with cancer (28) Now refers to an increase in number or size of seborrheic keratoses in patients with internal malignancy (24) Most often found in patients with adenocarcinoma of the stomach or colon (28) , but also reported with hematopoietic, breast, lung, ovarian, and uterine cancers (24, 29, 30) Can appear as early as 5 months before the dx of cancer or as late as 9.8 months after (29) Sign of Leser-Trelat Pathogenesis could be due to elevated levels of growth factors, disrupted epidermal cell turnover regulation, and impeded host defense (30) Treatment of the underlying malignancy results in involution of the SK’s in about ½ of cases (24,31) Hypertrichosis lanuginosa acquisita Sudden appearance of downy, soft, nonpigmented hair on the body Most common associated malignancy is lung followed by colorectal cancer (32) Also has been associated with bladder, ovarian, uterine, and pancreatic cancer (24, 33) Typically occurs on face, but also on trunk, limbs, and ears Palms, soles, and genitals are spared Can be associated with other signs and symptoms, including glossitis, glossodynia, diarrhea, adeopathy, and acanthosis nigricans In some cases, the hypertrichosis resolves with treatment of the tumor (24) Bazex’s Syndrome Violaceous, symmetric papulosquamous plaques on the acral surfaces of ears, nose, hands, and feet 75% have nail changes including longitudinal or horizontal ridging, thickening, subungal debris, and discoloration (24) Mostly male (93% in one study) (34) Associated with squamous cell carcinoma of the oropharynx, larynx, lung, or esophagus In one review, cutaneous changes preceded the diagnosis of malignancy by an average of 11 months in over 60% of patients with Bazex’s syndrome (35) Bazex’s Syndrome Violaceous, symmetric papulosquamous plaques on the acral surfaces of ears, nose, hands, and feet The dermatosis improves with cancer treatment and worsens as the cancer progresses (24) Nail changes tend to persist after effective cancer treatment and resolution of other skin manifestations Dermatomyositis Proximal muscle weakness, elevated CK and aldolase Heliotrope rash, Gottron’s papules, and others Some factors associated with higher incidence of paraneoplastic dermatomyositis Poikiloderma, periungual telangiectasia, scalp pruritis and erythema Older age, male gender, patients that are difficult to control Perform age-appropriate cancer screening for dermatomyositis patients 25% will develop malignancy (24, 35) , most commonly Genital neoplasms in women (24, 36) Respiratory tract neoplasms in men (24, 36) Heliotrope Rash in Dermatomyositis Heliotrope rash (violaceous erythema) of periorbital skin Gottron’s papules in Dermatomyositis Flat-topped, violaceous or erythematous papules on extensor surfaces Erythroderma Exfoliative dermatitis with a dramatic presentation characterized by widespread erythema and scaling of skin Often have lymphadenopathy, headaches, malaise, photosensitivity, and chills Pathogenesis is unknown, but may have to do with elevated cytokines and adhesion molecules causing increased epidermal turnover and exfoliation Many potential causes, including pre-existing dermatoses, drug rxns, and malignancy. Skin changes most commonly present before the diagnosis of malignancy is made. According to a study by Nicolis (37) , 20 out of 24 patients with erythroderma and mycosis fungoides, Hodgkin’s, or other lymphomas or leukemias had skin changes up to 25 years before the dx of cancer was made. Most often associated with lymphomas and leukemias (24, 37, 38, 39) Also been reported with liver, lung, thyroid, and prostate cancer (38) Erythroderma May begin as scattered erythematous pruritic patches that generalize with time Palms and soles usually spared Treat the underlying malignancy and use topical steroids. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Habif. Clinical Dermatology, 4th ed. Mosby Inc: 2004. Ferringer T, Miller F. Cutaneous manifestations of diabetes mellitus. Dermatol Clin. 2002; 20:483492. Perez MI, Kohn SR. Cutaneous manifestations of diabetes mellitus. J Am Acad Dermatol 1994; 30:519-31. Paron NB, Lambert PW. Cutaneous manifestations of diabetes mellitus. Prim Care 2000; 27:371-83. Nebesio C, Lewis C, Chuang T: Lack of an association between granuloma annulare and type 2 diabetes mellitus, Br J Dermatol 2002; 146(1):122. Studer E, Calza A, Saurat J: Precipitating factors and associated diseases in 84 patients with granuloma annulare: a retrospective study, Dermatology 1996; 193(4):364. Stuart CA, Gilkison CR, Smith MM, et al. Acanthosis nigricans as a risk factor for non-insulin dependent diabetes mellitus. Clin Pediatr 1998; 37:73-80. 0-Toole EA, Kennedy U, Nolan JJ, et al. Necrobiosis lipoidica: only a minority of patients have diabetes mellitus. Br J Dermatol 1999;140:283-6. Jelinek JE. Cutaneous manifestations of diabetes mellitus. Int J Dermatol 1994; 33:605-17. Sibbald RG, Landolt SJ, Toth D. Skin and diabetes. Endocrinol Metab Clin North Am 1996;25:46372. Goodfield MJD, Millard LG. The skin in diabetes mellitus. Diabetaologia 1988;31:567-75. Cruz PD. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol 1992;89:82S-5S. Huntley AC. The cutaneous manifestations of diabetes mellitus. J AM Acad Dermatol 1982;7:42755. References 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. Leonhardt JM, Heymann WR. Thyroid disease and the skin. 2002; 20: 473-481. Lindhoudt V, Schumacher Jr HR, Algeo S, et al. Scleromyxedema with myopathy and hyperthyroidism. J Rheumatol 1996;23:1299-301. Wu SL, Chang TC, Chang TJ, et al. Cloning and sequencing of complete thyrotropin receptor transcripts in pretibial fibroblast culture cells. J Endocrinol Invest 1996;19:365-70. Heymann WR. Cutaneous manifestations of thyroid disease. JAAD 1992;25:885906. Tosti A, Bardazzi F, Guerra L. Alopecia areata and thyroid function in children. JAAD 1988;19:1118-9. Wolf R, Feuerman EJ. Pemphigus in association with autoimmune thyroid disease. Cutis 1981;27:423-4. Bloch MH, Sowers JR. Vitiligo and polyglandular autoimmune endocrinopathy. Cutis 1985;36:417-9. Kato H, Uyeki Y, Kitajama Y, et al. A case of dermatomyositis and Hashimoto’s thyroiditis. J Dermatol 1988;15:273-5. Goh KL, Wang F. Thyroid disorders in systemic lupus erythematosus. Ann Rheum Dis 1986;45:579-83. Nicholson D, White S, Lipson A, et al. Progressive systemic sclerosis and Graves’ disease: report of three cases. Arch Intern Med 1986;146:2350-2. Boyce S, Harper J. Paraneoplastic dermatoses. Dermatol Clin. 2002; 20: 523-532. References 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. Cohen PR, Kurzrock R. Mucocutaneous paraneoplastic syndromes. Semin Oncol 1997;24:334-59. Sheperd M, Raimer S, Tyring SK, Smith E. Treatment of necrolytic migratory erythema in glucagonoma syndrome. J Am Acad Dermatol 1991;25:925-8. Thompson NW, Eckhausser FE. Malignant islet cell tumors of the pancreas. World J Surg 1984;30:324-9. Schwartz RA. Sign of Leser-Trelat. J Am Acad Dermatol 1996;35:88-95. Holdiness MR. The sign of Leser-Trelat. Int J Dermatol 1986;25:564-72. Safai B, Grant J, Good R. Cutaneous manifestation of internal malignancies (II): The sing of Leser-Trelat. Int J Dermatol 1978;17:494-5. Ellis DL, Yates RA. Sign of Leser-Trelat. Clin Dermatol 1993;11:141-8. Hovenden AL. Acquired hypertrichosis lanuginosa associated with malignancy. Arch Intern Med 1987;147:2013-8. Sindhuphak W. Vibhagool A. Acquired hypertrichosis lanuginosa. Int J Dermatol 1982;21:599601. Bolognia J. Bazex’s syndrome: acrokeratosis paraneoplastica. Semin Dermatol 1995;14:84-9. Gross G, Pfister H, Hellenthal B, et al. Acanthosis nigricans mailgna: clinical and virological investigations. Dermatologica 1984:168:265-72. Cox NH, Lawrence CM, Langtry JA, Ive FA. Dermatomyositis disease associations and an evaluation of screening investigations for malignancy. Arch Dermatol 1990;126:61-5. Nicolis GD, Helwig EB. Exfoliative dermatitis. Arch Dermatol 1973;108:788-97. Abrahams I, McCarthy JT, Sanders SL. 101 Cases of exfoliative dermatitis. Arch Dermatol 1963;87:96-101. Pal S, Haroon TS. Erythroderma: a clinicoetiologic study of 90 cases. Int J Dermatol 1998;37:104-7. References Photo references: www.dermatlas.org www.dermis.net www.emedicine.com Habif. Clinical Dermatology, 4th ed. Mosby Inc: 2004.