Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
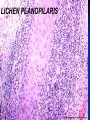
Mucinoses, Lichen Planus and Related Conditions Kristy P. Gilbert, D.O. January 24, 2006 What is Mucin? Fibrillar matrix in dermis called ground substance, created by fibroblasts. Ground Substance= acid glycosaminoglycans and proteoglycans (formerly called acid mucopolysaccharides) that bind 1000 times their own volume in water Adding sulfates to the acid GAGs creates chondroitin sulfate and dermatan sulfate, the 2 primary dermal mucins Classification Primary mucinoses Mucin deposition is the main histologic feature Secondary mucinoses Mucin deposition is an additional finding Examples include: LE, Dermatomyositis, Degos’, GA, cutaneous tumors, or after therapies such as PUVA or retinoids H&E: GA: Wispy bluish, feathery material between collagen bundles Colloidal Iron Staining: GA Mucin – “wispy, feathery” Mucin Stains Colloidal Iron Alcian Blue Toluidine Blue Incubation of tissue in hyaluronidase eliminates the staining, confirming the presence of mucin Lichen Myxedematosus Aka Papular Mucinosis Generalized = Scleromyxedema Onset age 30-80 Multiple waxy 2-4mm dome shaped or flat topped papules, usually linear array Acral: dorsal hands, face, elbows, and extensor extremities Five localized forms recognized. Characterized by a lack of monoclonal antibody and systemic disease. Lichen Myxedematosus Discrete Papular Lichen Myxedematosus Waxy 2-5mm firm flesh colored papules, usually confined to the limbs or trunk May have erythematous or yellow hue, and coalesce into nodules or plaques Slow accumulation of papules over time is the usual course Papular Mucinosis and AIDS Widespread Not associated with a paraprotein Always seen in advanced HIV disease If associated with eczematous dermatitis, usually clears when eczema clears May respond to oral retinoids Histopathology of lichen myxedematosus (discrete type). Mucin deposits splay collagen bundles in the dermis, but there is only slight fibroblast proliferation and no sclerosis. Lichen myxedematosus of the discrete type demonstrating mucin accumulation in the dermis. Alcian blue stain (pH 2.5). Acral Persistent Papular Mucinosis Subtype of localized LM Usually women- F:M ratio is 5:1 Few to 100 bilaterally symmetrical 2 to 5mm, flesh colored papules Almost always on hands and wrists. Rarely elbows, calves, or knees No paraprotein, no systemic disease H&E: Increased dermal mucin, but not fibroblasts Self-healing Juvenile Cutaneous Mucinosis Sudden onset, age 5 to 15 Skin lesions and polyarthritis x a few months. Ivory white papules head, neck, trunk and periarticular; also can be deep nodules on the face and periarticular regions Hard edema of periorbital area/face Acute arthritis affects the knees, elbows and hand joints TSH, IgG normal H&E dermal mucin Self-Healing Papular Mucinosis Adult form: Usually without the associated joint symptoms Prognosis of both forms is excellent with spontaneous resolution without sequelae over several months Cutaneous Mucinosis of Infancy AKA Papular Mucinosis of Infancy Subtype of localized LM 3 cases, onset birth-3 months of age 2-8mm skin-colored or translucent papules on trunk, extremities, especially backs of hands TSH, Paraprotein negative There are neither systemic symptoms nor spontaneous resolution as existing lesions remain static H&E: papillary dermal mucin, no fibroblast proliferation Generalized Lichen Myxedematosus Scleromyxedema Chronic and progressive; affects adults of both sexes usually from ages 30-80. Widespread eruption of 2-4 mm, firm, waxy, closely spaced dome-shaped or flat topped papules Papules often arranged in a linear array and may coalesce into plaques Surrounding skin is shiny and indurated(sclerodermoid) “Doughnut sign” = central depression surrounded by an elevated rim (due to skin thickening) is seen on the PIP joints. Scleromyxedema Woody, fibrous sclerosis of skin Lesions coalesce to form leonine facies Decreased ROM of hands, lips and extremities Dysphagia is most common GI symptom Scleromyxedema: Systemic Pulmonary Proximal Muscle weakness Arthralgias and inflammatory arthritis Carpal Tunnel Syndrome Peripheral Neuropathy Raynaud’s IgG lambda paraproteinemia Myeloma Scleromyxedema: Histopathology Triad Diffuse deposit of mucin in the upper and midreticular dermis Increase in collagen deposition Marked proliferation of irregularly arranged fibroblasts Increased fibroblasts and mucin in the reticular dermis Differential diagnosis Granuloma annulare Lichen amyloidosis Lichen planus Eruptive collagenoma Systemic scleroderma Scleredema Treatment Oral retinoids Systemic corticosteroids- low doses not usually helpful but high doses may temporarily arrest progressive visceral disease Extracorporeal photochemotherapy Melaphan Topical and intralesional hyaluronidase Electron-beam radiation Plasmapharesis PUVA Dermabrasion Topical DMSO Overall prognosis is poor. UVB and IFN alpha have exacerbated scleromyxedema Scleredema Stiffening and hardening of the subcutaneous tissues as if they were infiltrated with paraffin. With DM II (men); without DM II (women) Begins on the neck, may spread symmetrically to arms, shoulders and back- distal extremities spared Skin waxy, wood-like. Demarcation poor if no DM, good if DM Scleredema without DM II F>M 2:1, Poorly demarcated edges 25% Streptococcal infection Paraproteinemia usually IgG, Myeloma Cardiac arrhythmias. Upper GI dysphagia, tongue involvement Pleural, pericardial or peritoneal effusion If infection precedes it, 50% resolve 2-3 yrs. Cyclosporin, UVA1, pulsed dexamethasone, and extracorporeal photophoresis have been reported to be beneficial Scleredema with DM II Most common, well demarcated edges Associated with late-onset, insulin dependent diabetes M>F 10:1, usually obese Lesions insidious onset and long duration- MC mid upper back, neck and shoulders Sharp step off at lesion edge Persistent erythema & folliculitis possible Controlling DM II has no effect on skin No visceral disease or paraprotein Scleredema Clinical Photo Treatment PUVA Pulse therapy with cyclophosphamide and corticosteroids Electron-beam therapy Cyclosporine Therapy has little benefit, however Systemic and intralesional steroids, intralesional hyaluronidase, MTX, antibiotics, and penicillamine have not proved helpful REM Syndrome Reticular Erythematous Mucinosis Aka Plaque-like Cutaneous Mucinosis Women, 3rd -4th decades of life Frequently follows intense sun exposure, and often pregnancy, OCPs, menses DIF, ANA negative MC midline chest & back Reticulate or plaque-like appearance Antimalarials often helpful REM SYNDROME Cutaneous Focal Mucinosis Benign, symptomless, skin colored solitary lesions less than 1 cm Resemble neurofibromas, cyst, BCC, and angiomyxoma Can occur anywhere on the the body, except over the joints of the hands and feet Adulthood Histopathology: mucin throughout upper and middermis sparing subQ fat. Cleft like spaces, but no cysts, are seen. Numerous vimentin-positive dendritic shaped fibroblasts are seen Treatment: Surgical excision Follicular Mucinosis Aka Alopecia Mucinosa, 3 groups MC young; Occurs on the head, neck arms; resolves in 2 months to 2 years 2nd group, larger more numerous lesions, takes several years to resolve 3rd group, older, CTLC or lymphoma 30% of FM patients have MF Any patient >30 yo with FM, look for MF Follicular papules merging into a scaly plaque with alopecia MF associated follicular mucinosis H&E: asterisks mark large collections of mucin within cells of the sebaceous gland and outer root sheath with mixed dermal infiltrate Treatments for Follicular Mucinosis after you have ruled out MF: Topical or oral corticosteroids Dapsone PUVA, Radiation therapy Interferon alfa-2b Mepacrine Indomethacin Minocycline Oral isotretinoin Spontaneous involution may occur, especially in young children Myxoid Cysts MC terminal dorsal or lateral fingers Solitary 5-7mm opalescent or skin colored asymptomatic swellings of proximal nail fold or DIP NO CYSTIC LINING, not a true cyst Synovial origin still debated TX: I&D, Cryo, IL steroids, fulguration of the base after draining, CO2 laser ablation. Recently recognized association of multiple myxoid cysts with connective tissue disease i.e. JRA and systemic sclerosis. •Groove of nail plate secondary to lesional pressure to the nail matrix Case of dermatomyositis presenting with cutaneous mucinosis as the sole manifestation. A malignancy screen revealed an underlying nasopharyngeal carcinoma. (J Am Acad Dermatol 2003;48:S41-2.) Lichen Planus and Related Conditions Lichen Planus A disease of the skin, nails, hair follicles and mucous membranes. Mnemonic the 5 P’s Wickham’s Striae, flat topped papules Pruritis is paroxysmal, rubbing > scratching Flexor wrists, trunk, medial thighs, shins, dorsal hands, glans penis Plentiful Purple Pruritic Polygonal Papules Wickham’s striae: gray or white puncta or streaks that cross the lesion 5-10% of LP cases have nail changes including pterygium, longitudinal grooving, onycholysis, splitting and peculiar midline fissure Oral LP 75% of pts are women 15% also have skin lesions Ulcerative Reticulate Atrophic MC on buccal mucosa Risk of SCC 1/200 cutaneous LP pts develop oral SCC MC in ulcerative or erythematous lesions Mouth, anus are risk areas too. A - Annular LP – most commonly found on lips or penis. Central hyperpigmentation is characteristic Bullous LP Usually shins, as individual lesions merge, they vesiculate centrally. Often resolves spontaneously Lichen Planus Pemphigoides Rare Typical LP patients who experience bullae on top of their LP plaques Pruritis may be severe Triggered by medications and PUVA DIF positive for 180kd BPAg2 antigen Treat like Bullous Pemphigoid- potent topical or systemic steroids, TCN, Nicotinamide, IVIG, immunosuppressives Hypertrophic LP AKA: LP verrucosus Extremely pruritic Usually symmetric, MC on shins Chronic venous stasis frequently contributes to this condition, making lesions refractory SCC, which must be distinguished from pseudoepitheliomatous hyperplasia, has been reported to arise within these lesions Hypertrophic LP Linear LP – Aka Zosteriform 1% of LP cases Blaschko’s lines, not dermatomal MC in children Hepatitis C Prevalence in LP pts between 4% and 38% Japan: Hep C = 8%, LP w/ HepC = 60% LP patients with Hep C are more likely to have erosive mucous membrane dz. TX of Hep C w/ Alpha INF may induce LP. Primary biliary cirrhosis & LP may coexist; ↑ risk of lichenoid rxn to D-Penicillamine HBV immunization also associated- more than 30 cases reported Lichen Planopilaris - scalp only Graham-Little-Picardi-Lasseur Syndrome - scalp & hairbearing body sites Females > Males 4:1 Tufts of normal hair appear in cicatricial areas of alopecia Perifollicular erythema and keratotic spiny papules Tx: Difficult, IL or oral steroids, antimalarials. Interface dermatitis with “saw-tooth” pattern of epidermal hyperplasia together with orthokeratosis and hyper-granulosis. Basal layer is lost or “squamatized” with vacuolar interface change, necrotic keratinocytes. “Band-like” infiltrate in the papillary dermis. “Civatte bodies” are necrotic keratinocytes in the dermis Hyperkeratosis, irregular (saw-tooth) acanthosis, dyskeratosis, basal vacuolization, and a band-like infiltrate of mononuclear cells Hyperkeratosis, focal increase in the granular layer, saw toothing of the epidermis and a lichenoid infiltrate. LICHEN PLANOPILARIS LP Pathology Hypertrophic LP = LP + LSC LPP and GLPL = LP histology centered on follicular epithelium Civatte bodies reveal IgM on DIF Lichenoid drug reaction may mimic LP. Look for eosinophils, photodistribution to distinguish. Lichen Planus Treatment Prednisone, Isotretinoin PUVA, LMW Heparin, Cyclosporin Oral: potent topical steroids in Orabase w/ vinyl dental tray TID and 20 mins qHS Plaquenil 400mg daily Inhaled forms of corticosteroid are sometimes helpful for oral LP Vaginal: mix steroids with Replens (bioadhesive moisurizer) Hydroxychloroquine, thalidomide have also been used Mycophenolate mofetil and cyclosporin for refractory cases. Lichen Planus Actinicus MC Africa, Middle East, Indian, Asians MC Spring, Summer, Quiescent in Winter Photodistributed Mild or no pruritis Hyperpigmented macules or plaques with the blue-gray tinge of dermal melanin May resemble Melasma Erythema Dyschromicum Perstans Onset before age 40. Chronic generalized, symmetrical Various sizes & shapes, ashy-gray macules, sometimes with a palpable non-scaling border. Feels “like a small cord” Pruritus is not reported Nail and mucosal involvement is not found Erythema Dyschromicum Perstans Erythema dyschromicum perstans Occasionally there is a peripheral rim of erythema As in pityriasis rosea, the long axis of oval lesions can follow skin cleavage lines Histology: lichenoid infiltrate with pigment laden macrophages in the dermis EDP Treatment Sun protection Topical retinoids Topical vitamin C Chemical peels Oral antibiotics Oral vitamin A Dapsone Antimalarials Griseofulvin Anecdotal report with clofazamine Systemic and topical steroids Lichenoid Contact Dermatitis Dorsal hands - Paraphenylenediamine (color film) Oral due to Amalgan fillings Patch testing recommended Keratosis Lichenoides Chronica Rare, acral & buttocks, onset childhood Violaceous papulonodular, hyperkeratotic lesions covered with gray scales; discrete or may coalesce to form reticulate or linear arrays, keratotic plugs and prominent telangiectasias Associated facial “seb derm” pattern Nail thickening, longitudinal ridging, onycholysis, warty periungual lesions Painful oral apthae, keratoconjunctivitis Tx: symptomatic; usually unsatisfactory Keratosis Lichenoides Chronica Lichen Nitidus Minute, shiny, flat-topped, pale, exquisitely discrete, uniform papules Lichen Nitidus – H&E CHARACTERISTIC PATH: EPIDERMIS GRASPS LYMPHOHISTIOCYTIC INFILTRATE WITH “CLAW-LIKE COLLARETTE LICHEN NITIDUS Lichen Nitidus Linear Koebnerization Lower abdomen and penis, inner thighs, flexor wrists and forearms Actinic Lichen Nitidis in black, Middle Eastern and Indian subcontinent Slowly progressive with tendency to remissions Tx: Top. Steroids, PUVA, DNCB, Oral Retinoids Lichen Striatus Common, Linear, erythematous or hypopigmented papules, scaly, asymptomatic, follow Blaschko’s lines, nails may be involved Children age 3, females > males Active lesions last for months, then resolve Histology varies, lichenoid or spongiotic, possibly even granulomatous. Dense eccrine infiltrate helps differentiate from LP Lichen Sclerosis et Atrophicus Females > Males, Itching may be severe Anogenital “hourglass” or “figure eight” with dyspareunia Glans penis (balanitis xerotica obliterans) Chest, breasts, back, oral mucosa, tongue Histology may have features of morphea Genital SCC risk higher than general population, but lifetime risk is < 5% LS&A IN A PERIUMBILICAL SKIN FOLD LS&A Etiology Unknown. Borrelia burgdorferi assoc. Japan, Europe 20% of pts have autoimmune disease, usually vitiligo, alopecia areata or thyroid LS&A Treatment Steroids (clobetasol) Topical testosterone (emollient) Topical retinoids CO2 laser ablation Excisional bx Oral calcitriol (used in morphea and scleroderma) Pimecrolimus/tacrolimus PDT Topical estrogens Childhood LS&A Childhood onset in 10-15%, usually genital Boys present with phimosis, circumcision may improve/resolve Girls present with pain with defecation, dysuria and 50% have spontaneous resolution LS&A Histology LATE LS&A: RETE RIDGES EFFACED, EDEMA “FADED, WASHED OUT LOOK”, TELANGIECTATIC VESSELS JAAD, Volume 48, Number 6: Pages 935-937, June 2003 Tacrolimus ointment for the treatment of vulvar lichen sclerosis. Assmann T, Becker-Wegerich P, Grewe M, Megahed M, Ruzicka T. Department of Dermatology, Heinrich-Heine-University, Düsseldorf, Germany. The treatment of vulvar lichen sclerosus is generally considered difficult. Ultrapotent corticosteroids represent the most effective topical treatment, but carry the risk of side effects such as skin atrophy. We describe a 71-year-old woman with long-standing vulvar lichen sclerosus refractory to conventional treatment. After 6 consecutive weeks of treatment with tacrolimus ointment 0.1% (Protopic) twice daily, signs and symptoms of lichen sclerosus resolved. To our knowledge, this is the first report of the use of topical tacrolimus, which does not induce skin atrophy, in the treatment of vulvar lichen sclerosus. PMID: 12789187 [PubMed - indexed for MEDLINE] The End