Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
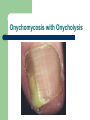
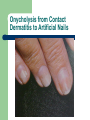
Fungal Infection of the Skin November 24th , 2003 Michael Hohnadel D.O. Duncanville Dermatology Clinic Dermatology Residency KCOM Dermatology Department Topics Covered Basic diagnostic techniques – – – KOH Culture Woods light Tinea infections with special attention to scalp, feet and nails Tinea Versicolor Candidiasis Differentials to consider. Basic Treatment Questions 1. What is a Wood’s light useful for ? 2. If I think it might be a fungus but it is KOH negative, what can be done to prove it ? 3. How do you know the endpoint of therapy when treating tinea capitis ? 4. How do you know the endpoint of therapy when treating tinea versicolor ? 5. If a patient has thick ugly nails, what is the chance that it is classic onychomycosis ? Diagnostic Tests KOH Preparations Skin – – – – Two slides or slide and #15 blade. Scrape border of lesion. Apply 1-2 drops of KOH and heat gently Examine at 10x and 40x – Look for hyphae – Focus back and forth through depth of field. Clear, Green Cross cell interfaces Branch, constant diameter. Chlorazol black, Parkers ink can help. Diagnostic Tests KOH Preparations Nails – – – – Hair – – – Thin clipping, shaving or scraping Let dissolve in KOH for 6-24 hours. Can be difficult to visualize. Culture often required. Directly examined without KOH. Apply KOH and heat hair until macerated Look for spores. Be Persistent ! Tinea Versicolor Trichophyton Tonsurans Tinea Versicolor Parkers Ink Stain Watch out for Mosaic Fungus Mosaic Fungus Lipid droplets in interepithelial spaces and cell membrane overlap simulate fungal hyphae. Diagnostic Tests Fungal Cultures DTM (Dermatophyte – Yellow to red is (+). Nickerson’s Media – Yeast – Black growth is (+) Sabouraud’s – Molds Media Test Medium) Diagnostic Test: Fungal Culture Example of DTM Diagostic Test Fungal Culture Diagnostic Tests Fungal Culture Sample Collection Scrape with blade or rub with cotton Q-tip. Nail clipping or curette. Implant in media. Cap Loosely, Fungi are aerobic Read at 2 weeks and 4 weeks. Tinea Capitis Diagnostic Tests Wood’s Light – Tinea Capitis – Other Areas: Blue green florescent with M. Canis. Not useful for Trichophyton (Most Common) Useful to diagnose as erythrasma (coral red/pink). Tinea versicolor may be pale white yellow. Less helpful if patient recently bathed. PAS stain of skin or nail clipping. Woods Light – M. Canis Woods Light - Erythrasma Different Types of Infection Dermatophyte Fungal Infection – Tinea Capitis – Tinea Pedis – Tinea Unguium (Onychomycosis) – – – – Tinea Corporis Tinea Faciales Tinea Cruris Tinea Manuum Tinea Vesicolor Candidiasis Tinea Capitis Tinea Capitis • Children most common cases. • Most Common Organisms: • T. Tonsurans - acounts for 90% in U.S. • M. Canis - seen in children with infected animals. •Adults not infected. • M. Audouinii - grey, broken shaft tinea Tinea Capitis Presentations of Tinea Capitis 1. Non-inflammatory ‘black dot’ type 2. Seborrheic type 3. Pustular 4. Inflammatory (Kerion) Tinea Capitis Black Dot Type Large Areas of Alopecia without inflammation Mild scaling Occipital adenopathy Black dot hairs. At first glance may look like Alopecia areata Tinea Capitis Tinea Capitis Seborrheic type Common– resembles dandruff Close exam for broken hairs, black dots Adenopathy Frequently negative KOH (70%) Culture often necessary for DX Tinea Capitis Kerion Inflamed, Boggy and tender. M. Canis common etiology Systemic symptoms: Fever, Adenopathy. Scaring alopecia may occur KOH often negative May look bacterial Tinea Capitis - Kerion Tinea Capitis Pustular •Discrete pustules and crusted areas •No significant hair loss or scale •Often KOH negative •Frequently treated as bacterial at first Tinea Capitis Diagnosis History Morphology of lesion Blue green. Hair Shaft Exam Broken hairs, black dots, localized. Woods Lamp Close contacts, pets, duration. Endo/Exothrix Culture Plucked Hair shafts, Q-tip or tooth brush. Normal Hair Tinea Capitis - Endothrix Tinea Capitis - Exothrix KOH and ‘Quick Ink’ M. Canis Tinea Capitis Treatment •Must treat hair follicle •Topical not effective •Systemic agents •Griseofulvin for children – liquid with good taste. •Imidazoles, terbinafine. •Steroids for inflamed lesions like Kerion. •Treat until no visual evidence, culture (-)… plus 2 weeks •Average of 6-12 weeks of treatment. •Examine / treat family in recurrent cases. Tinea Pedis and Manuum. T. Rubrum most common etiology •Dull erythema with pronounced scale. •Leading edge of scale not as common. •Two feet one hand involvement. •T. Mentagrophytes causes inflammatory tinea pedis •Vesicles and bullae. General Morphology Tinea Pedis Tinea Pedis General Morphology Tinea Manuum Two feet one hand Tinea Pedis •Groups: M > F. Young and middle aged. •Patient is susceptible to reoccurrence •Onychomycosis and tinea pedis associated. •Differential: •Eczema, contact dermatitis •Psoriasis. •Erythrasma and Candida (esp in web spaces.) •Pitted keratolysis Tinea Pedis Diagnosis •PE/History – onychomycosis, contacts, med cond. •KOH exam – Thick scale, no leading edge •Woods Light - Helps to differentiate from erythrasma •Culture •Remember: ‘hand eczema’ may be a dermatophyte infection of hands or id reaction from tinea at another location. Tinea Pedis: Treatment •Dry Feet •Alternate shoes, Absorbent powders, Change socks •Scale my be reduced with keratolytic •SAL acid, Lactic acid, Carmol •Topicals and/or Systemics. •Topical: naftine, lamisil, mentax may be more effective than azoles. Steroids if inflamed. •Systemic allyamines or azoles •Treat secondary bacterial infections. •Steroids for severe inflammation and ID. General Morphology Onychomycosis 15-20% of those between 40-60 yrs. infected. No Spontaneous remissions General Appearance: – – – – – – Typically begins at distal nail corner Thickening and opacification of the nail plate Nail bed hyperkeratosis Onycholysis Discoloration: white, yellow, brown Edge of the nail itself becomes severely eroded. Some or all nails may be infected Often accompanying tinea pedis Onychomycosis 4 Types: 1. 2. Distal Subungal White superficial 3. Proximal Subungal 4. T. Mentagrophytes and molds Chalky white patches May indicate HIV infection Candidaonychomycosis Normally hands with accompanying paronychia Onychomycosis Onychomycosis with Onycholysis White Onychomycosis Candidaisis of nail Paronychia Onychomycosis Differential Diagnosis: (50% of ‘thick nails’ not classic fungus.) •Allergic contact (nail polish, food items) •Psoriasis •Lichen Planus •Molds •Nail dystrophies (ex – nephrogenic) •Drugs Onycholysis from Contact Dermatitis to Artificial Nails Psoriasis Middle of nail, oils spots, pitting. Psoriasis Lichen Planus Onycholysis from wet - dry Pseudomonas of nail Terry nails ‘half and half’ Molds Bowen’s disease of the Nail Onychogryphosis Diagnosis of Onychomycosis Try to identify fungi before oral therapy 1. KOH of nail clipping • May need some time to dissolve nail. 2. Culture • DTM - dermatophytes • Sauborauds – Molds • Nickerson – Yeast 3. Nail clipping for histology and PAS staining if above is negative and clinical suspicion is high. Curettes for Specimen Collection. Treatment of Onychomycosis. Debridement of infected area helps penetration / comfort. • Mechanical • Urea products (ex carmol) Topical Treatment: • Can be effective for limited involvement and for prevention. • Agents • Penlac (every day for one year) • Mycocide Nail solution Treatment of Onychomycosis Oral therapy •Effective. Relapse rate 15-20 % in one year. •Lamisil 250mg. 6 weeks/12 weeks. •Baseline labs and one month. •CBC (neutropenia), Liver function. •Itraconazole 200 mg /day. 6 weeks/12 weeks •Baseline labs and one month. Similar to lamisil. •Pulse dosing fingernails - (200 mg bid 1 wk q mo.) x 2 •No lab monitoring needed Treatment of Onychomycosis Notes on Therapy • Other Azoles require longer therapy. • Nails will not appear clear at end of therapy • Measurements and digital photography verify effectiveness. • For you and for patient General Morphology Tinea Corporis Papulosquamous Erythematous Annular Scaling Crusting ‘Ringworm’ General Morphology Tinea Faciales General Morphology Tinea Cruris General Morphology Tinea Versicolor Numerous, well-marginated, oval-to-round macules with a fine white scale when scraped. Pigmentary alteration uniform in each individual. – – – Scattered over the trunk and neck. Seldom the face. Pityrosporum orbicularis, M. furfur – Red Hypo pigmented Hyperpigmented Normal flora of skin Asymptomatic. Tinea Versicolor More apparent in the summer. Tinea Vesicolor Hyperpigmented Variety Looks Like: intertrigo, erythrasma …. Tinea Versicolor - Differential •Vitiligo •Pityriasis Alba •Pityriasis Rosea •Nummular Eczema •Psoriasis •Idiopathic guttate hypomelanosis Vitiligo White without scale. Pityriasis Alba Frequently on face, KOH neg. Few lesions. May have fine white scale. Pityriasis Rosea •Papules or plaques with Collarette of scale, KOH (-), Woods light neg. HX. Guttate Psoriasis Idiopathic guttate hypomelanosis •White, small, no scaly, age. Tinea Versicolor Diagnosis: •Scrape lightly – fine white scale •KOH Positive for short hyphae and spores (Spaghetti and meatballs) •Woods Light – pale yellow white fluoresce. •Culture rarely done. Tinea Versicolor Tinea Vesicolor – Woods Light Yellow White Tinea Versicolor Microscope Tinea Versicolor-Treatment Topicals for limited involvement. •Selenium Sulfide Shampoos: lather 10 minutes wash off x 7 days. •Ketoconazole 2% shampoo: 5 minutes 1-3 days. •Imidazoles topicals to body qd-bid for 2-4 wks. •Terbinafine spray. Tinea Versicolor-Treatment Oral for extensive •Itraconazole, fluconazole, ketoconazole. •Dosing varies: single dose to 5-10 days of therapy. •Likes gastric ph for absorption. •Avoid bathing with 12 hours of ingestion. Tinea Versicolor-Treatment Notes •Hypopigmentation resolves slowly •No scale when scraped indicates cure. •Sunlight helps restore pigment •Prophylaxis before summer in some patients. •Selenium shampoo’s •Q month orals Candidiasis •Candida Albicans •Normal Flora •Occurs in moist areas especially where skin touches. •Presentation: primary lesion is a red pustule. •Most Common: pustules dissect horizontally through the stratum corneum leaving a red, glistening denuded surface with long continuous border with satellite lesions. •May also present as an eruption of multiple pustules which become erythematous papules between skin folds. Candidiasis •Immunosuppression of any type (disease, steroids), D.M., Antibiotics or receptive environments predispose. •Diagnosis: History of predisposing factors and/or classic appearance of lesions at typical locations. •Red and glistening in intertriginous area esp in predisposed individual think candida. Candidiasis Candidiasis Difficult to be sure in Web spaces. Candidiasis Differential: 1. Erythrasma – likes skin creases 2. Eczema – may look like pustular candida 3. Bacterial folliculitis – as above 4. Psoriasis – gluteal cleft 5. Tinea – same locations Candidiasis •KOH for pseudohyphae and spores •May be impossible to tell visually from tinea. •Woods Light •Culture. Nickersons (+) •Remember yeast part of normal flora. •Add up the evidence Candidiasis Treatment of Candidiasis • Keep dry – Z-sorb powder, cotton ball between toes. • Topical – azoles. • Occasionally co-administration of a weak topical steroid may be helpful. • • Diaper rash • Angular chelitis. Treat co-existent bacterial infection if present. THE END