Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
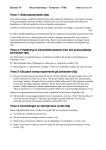
MİYASTENİA GRAVİS Prof.Dr.Aytekin Akyüz CÜ Tıp Fak Nöroloji AD MİYASTENİA GRAVİS (MG) ► Nöromüsküler kavşak hastalıklarının (MG, botilismus, Lambert-Eaton Sendromu) en sık görüenidir. ► Çizgili kaslarda postsinaptik membrandaki nikotinik tipte asetilkolin resptörlerine karşı antikor oluşumu ile karekterize otoimmün bir hastalıktır. MOTOR END-PLATE or NEUROMUSCULAR/MYONEURAL JUNCTION AXON SCHWANN CELL AXOLEMMA SARCOLEMMA SYNAPTIC VESICLES mitochondrion synaptic cleft secondary/ junctional folds of POST-SYNAPTIC MEMBRANE SKELETAL MUSCLE FIBER/MYOCYTE MOTOR END-PLATE: LOCATION OF ‘TRANSMISSION’ MOLECULES SARCOLEMMA voltage-gated ion channels AXOLEMMA voltage-gated ion channels Acetyl Choline/ACh SYNAPTIC VESICLES synaptic cleft Cholinesterase PRE-SYNAPTIC MEMBRANE Ca2+ channels Ligand-gated ion channels ACh receptors POST-SYNAPTIC MEMBRANE SKELETAL MUSCLE FIBER/MYOCYTE NMJ Normal nöromusküler kavşak modeli. Nerve aksiyon potensiyelinin sinir terminaline ulaşması, asetilkolin salınımını artırışı. Solda normal nöromusküler kavşak ile birlikte sağda miyastenik nöromusküler kavşak MG ► Prevelans 1-15/100.000 ► Kadın/erkek 3:2, kadında 2-3. dekat, erkekte 50-70yaş daha sık ► Egzersizle ortaya çıkan, istirahatle düzelen kuvvet kaybı tipiktir ► %60-70 ptoz ve ekstraoküler kas tutulumu ile başlar Egzersizle ortaya çıkan, istirahatle düzelen kuvvet kaybı Seri çekilmiş 3 resim sürekli yukarı bakan hastada göz kapağı kaslarında yorulma ve güçsüzlüğü gösteriyor Birkaç dakika istirahattan sonra göz kapaklarının hemen hemen normale dönmesi MG semptomları istirahat ile düzelir Tensilon öncesi ve sonrası MG Klinik Tipleri ► Oküler miyastenide sadece ekstraoküler kaslar tutulur ► Jeneralize miyastenili hastalar oküler, fasiyal, çiğneme kasları, orofaringeal, respiratuvar (1/3) ve ekstremite kasları (proksimalde belirgin) tutulumu sonucu fluktüasyon gösteren çift görme, göz kapağında düşme; çiğneme, yutma ve konuşma güçlükleri, ses kısıklığı; solunum sıkıntısı ve güçsüzlük şikayetleri ile başvurur. ► Oküler miyasteni %10 jeneralize miyasteni %90 oranında görülür ► Olguların %70 inde timik displazi, %1015’inde timoma görülür. ► Romatoid artrit, SLE, pernisiyöz anemi, tiroid hst.,vitiligo gibi diğer otoimmün hastalıklarla birlikteliği sıktır. Tanı ► Anamnez Günün ilerleyen saatlerinde veya egzersizle pitoz çift görme vs ortaya çıkması, istirahatle ve sabah semptomların düzelmesi ► Yorma testi Egzersizle ptoz, bakış kısıtlılığı veya kuvvet kaybı oluşması. Ör. 2 dk. yukarı bakışla ptoz ve yukarı bakış kısıtlılığı ► Buz testi Bir buz torbasının göz üzerine 2 dk konması ile ptoz ve bakış kısıtlılığının düzelmesi Tanı (2) ► Tensilon (veya prostigmin) testi (asetilkolinesteraz inhibitörleri ile semptomların düzelmesi oküler MG’de %50, jeneralize MG’de %70 (+) dir. ► Elektrofizyolojik Testler Ardışık (repetetif) uyarımla “dekrement yanıt” (%75) Tek Lif EMG’de “artmış jitter” (%98-100) ► Antikor tespiti anti-AchR Ak (jeneralize %90, oküler %70 +) antistriational Ak (MG+timomada %80) Repetetif (ardışık) Uyarımla KAP Repetetif (ardışık) Uyarımla Dekrement Yanıt ► Dekrement yanıt (>%10) RNS ► Decrement in CMAP amplitude ► Post-exercise exhaustion ► Post-tetanic potentiation Tek lif EMG - jitter Tek lif EMG ► Normal ► ► anormal ► MG düşünülen hastalarda timus patolojisi (CT,MRI) ve diğer otoimmün hastalıkların varlığı araştırılmalıdır. Miyastenik Kriz ► ► Respiratuvar (diyafragma, interkostal) ve orofaringeal kaslarda parezi/paralizi sonucu aspirasyon ve solunum arresti görülebilir (%15-20). Presipitan Faktörler stress, ağır ekzersiz, tedavi şemasında değişiklik, infeksiyon (%38), ilaçlar (antibiyotik, antiepileptik, antiaritmik, Dpenisillamin), operasyon, hamilelik-doğum ► ► 1/3’ünde presipitan faktör yok Semptomlarda kötüleşme varsa solunum ve bulber güçsüzlük takibi!! dispne, hızlı-parodoks solunum, yutma güçlüğü, aspirasyon!!! ► ► Bir inspiryumla sayı sayma (>50) Hospitalize MG krizli hastalarda %10 mortalite MG’yi kötüleştiren ilaçlar ► Antibiyotikler (Sefalosporinler hariç) ► KVS ilaçları (β blokör, antiaritmik) ► SSS etkili ilaçlar (antiepileptik) ► Antiromatizmal ajanlar ► Diğer (Steroid, Mg, lokal anestezik) Tedavi ► Asetil kolinesteraz inhibitörleri Prostigmin Pridostigmin (Mestinon) ► Kortkosteroidler veya diğer immünosupresif ajanlar Prednison 15-20mg/gün başlanarak 1mg/kg/ güne çıkılır ► Plamoferez dolaşımdaki IgG ve AchR antikorlarının azaltılmasını sağlar ► IVIG ► Timektomi displazi varsa jeneralize MG’de, timoma varsa tüm miyasteniklerde Miyopatiler ► ► ► Largest group of neuromuscular diseases Most diverse group All show a loss of muscle fibers Proximal more than distal ► No involvement of the anterior horn cell, nerve axon, or neuromuscular junction Miyopatiler ► Includes ► 1. ► 2. ► 3. ► 4. ► 5. ► 6. 6 subcategories Endocrine Disorders Metabolic Disorders Myotonias Periodic Paralysis Polymyositis Muscular Dystrophy Endocrine Disorders ►• Myopathies caused by some malfunction of the endocrine system ► • Chronic ► • Examples: – Addison’s Disease – Cushing’s Syndrome – Thyrotoxic Myopathy ► • Respond to drug therapy – Consists primarily of replacing the deficient hormones Metabolic Disorders Myopathies characterized by a deficiency of a specific enzyme resulting in muscle weakness ► Examples: ► McArdle’s Disease: Deficiency of the muscle enzyme myophosphorylase Pompe’s Disease: deficiency in Acid Maltase Miyotoniler ► Hereditary myopathies ► Result of a chromosomal mutation ► Characterized by: Inability to relax a previously contracted muscle ► Elicited by either voluntary contractions or some external stimuli such as percussion ► Worsened by cold ► Lessened by light exercise ► Examples: Myotonic Congenita (Thomsen’s Disease) Myotonia Atrophic Miyotonik Distrofi (Steinert’s Disease) ►– Most frequent neuromuscular disease although it is relatively rare ► – Clinical signs and symptoms: Atrophy Weakness Involvement of the more distal muscles such as: ► – Face – Neck– Tongue – Intrinsics of hands and feet Miyotonik Distrofi Myotonic Congenita (Thomsen’s Disease) ► Children develop a characteristic hypertrophy of the: Neck Deltoid Biceps Triceps Quadriceps, and Gastrocnemius muscles – Child appears to be a “Tiny Hercules” Miyotonia Congenita Periodic Paralysis ► ► ► Relatively rare myopathy Hereditary – Autosomal dominant Characterized by: Transient flaccid paralysis or paresis affecting primarily the muscle of the proximal limbs Attacks of weakness may last from a few seconds to several weeks Involvement of a disruption in the serum K+ balance ► Examples: Hyperkalemic Form Hypokalemic Form Hiperkalemik Form Has increased serum K+ ► Triggered by: ► ► Stress Fasting Cold Rest following intensive or prolonged muscular exercise Attacks minimized by: Light exercise Ingestion of carbohydrates Hipokalemik Form Has decreased serum K+ ► Affects men more than women ► Triggered by: ► Stress Fasting Cold Rest following intensive or prolonged muscular exercise Alcohol consumption High carbohydrate diets Polimiyozit Second most common myopathy in adults ► Chronic inflammatory condition of striated muscle ► Skin involved 50% of time – In this case its called Dermatomyositis ► Insidious onset ► Moderately progressive ► Clinical signs: ► Muscle weakness Fatigue Flexors more than extensors Difficulty swallowing Joint pain Mild fever Weight loss Very diffuse erythema of face and neck Müsküler Distrofi ► ► ► Largest group of the myopathies Group of inherited diseases Characterized by: Progressive muscle weakness Müsküler Distrofi ► Pseudohypertrophic Muscular Dystrophy (Duchenne’s) ► – Becker-type Muscular Dystrophy ► – Facioscapulohumeral Muscular Dystrophy ► – Limb-girdle Muscular Dystrophy Duchenne’s Muscular Dystrophy Also known as Pseudohypertrophic Muscular Dystrophy ► Most common and most devastating dystrophy ► X-linked ► Therefore, only affects males ► ► Progressive Rare for patients to live to the age of 30 Duchenne’s MD ► Clinical signs and symptoms: Marked elevation in serum Creatine Kinase Psuedohypertrophy of the calves Tightness of the achilles Hyperlordosis in the low back Progressive atrophy and weakness of the pelvis and LEs Gover’s sign Becker-type Muscular Dystrophy ► ► ► ► More benign form of Duchenne’s Found more in older children Progresses much slower Children live to reach adulthood Emery Dreifuss MD Facioscapulohumeral Muscular Dystrophy Autosomal dominant ► Involves teenagers ► Pattern of muscle weakness in face and shoulder girdle ► FSHD Limb-girdle Muscular Dystrophy Autosomal recessive ► Affects ages 20 – 30 ► Pattern of muscle weakness of the proximal pelvic muscles and shoulder girdle ► Neuromuscular Junction Disorders Defect in the transmission of the neurochemical signal across the neuromuscular junction ► Defect can take form of a problem in: ► Release of acetylcholine (Ach) Uptake of Ach, Insufficient receptor sites at the junction Neuromuscular Junction Disorders Categorized as pre-synaptic or post-synaptic problem ► Examples: ► Myasthenia Gravis ► Post-synaptic receptor site disorder Myasthenia Syndrome ► Pre-synaptic calcium channel disorder Lambert-Eaton Syndrome Botulism ► Toxin prevents pre-synaptic release of Ach Clinical picture: ► Clinical ► ► picture: Pronounced, rapid fatigue Associated muscle weakness Strength may be normal with a single repetition Repeated contractions lead to rapid fatigue PARANEOPLASTIC SYNDROMES Arti Balar Masturzo, MD November 17, 2003 DEFINITION disorders caused by cancer but not due to metastatic disease or nonmetastatic mechanisms IMPORTANCE early detection of cancer ► save $$ in work-up OBJECTIVES • DISCUSS 3 TYPES OF PNS – NERVOUS SYSTEM – CUTANEOUS – RHEUMATOLOGIC • DISCUSS KNOWN MECHANISMS • CORRELATE WITH CLINICAL CASES PNS OF THE NERVOUS SYSTEM PATHOGENESIS • IMMUNOLOGIC FACTORS • ABNORMALTIES DUE TO HORMONE/CYTOKINES HYPONATREMIA HYPERCALCEMIA HYPOGLYCEMIA – • TUMOR VS. NERVOUS SYSTEM • • IMMUNOGLOBULIN SYNTHESIS – ► DIAGNOSIS ►MAY DEVELOP BEFORE TUMOR Dx ►HIGH INDEX OF SUSPICION ► Dx OF EXCLUSION ►SPECIFIC TESTS MAY BE HELPFUL ►NEUROIMAGING ►CSF STUDIES ►ELECTROPHYSIOLOGY ►PET SCAN ► PNS OF THE NERVOUS SYSTEM ► CENTRAL NERVOUS SYSTEM ► PERIPHERAL NERVOUS SYSTEM ► NEUROMUSCULAR JUNCTION & MUSCLE 53 yo male smoker presented with agitated behavior, drowsiness, confusion, hallucinations, loss of memory, and multiple generalized tonic clonic seizures. CXR shows left hilar mass MRI: enhancement in temporal lobes and parahippocampal gyri CENTRAL NERVOUS SYSTEM • • • • • • • • LIMBIC ENCEPHALITIS MYELITIS ENCEPHALOMYELITIS BRAINSTEM ENCEPHALATIS CEREBELLAR DEGENERATION OPSOCLONUS MYOCLONUS ATAXIA NECROTIZING MYELOPATHY VISUAL SYNDROMES – CANCER ASSOCIATED RETINOPATHY – MELANOMA ASSOCIATED RETINOPATHY – OPTIC NEURITIS