Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
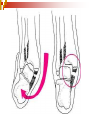
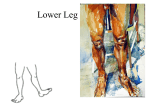
The Ankle & Lower Leg Lecture 10 Lower leg and ankle ankle injuries most frequent in sports tibia is major weight bearing bone of the lower leg fibula assists minimally with weight bearing aprrox 2 % , serves as a site for muscle attachment and contributes to the stability of the ankle Crural Bones med / lat. malleolus and talus Talocrural Joint (ankle joint) is a uniaxial modified hinge joint - (talus, tibia and fibula) plantar flexion and dorsiflexion occur here talus wider ant vs post stability Lateral Ankle Support ATF, PTF , CF (static) (AITF) b) peroneals (dynamic) the lateral ligaments of the ankle joint are relatively weaker than the medial ligaments hence the larger number of lateral ankle sprains a) Medial Ankle a) Deltoid ligament (static) b) Tom, Dick and Harry (dynamic) Dynamic TA TP Distal Tib-Fib Joint a) ant & post tibiofibular lig b) interosseos membrane Muscles 4 compartments anterior , deep , superficial and lateral i) anterior - tibialis anterior - extensor digitorum longus - extensor hallucis longus and peroneous tertius ii) deep - tibialis posterior - flexor digitorum longus - flexor hallicus longus iii) superficial - gastrocnemius - soleus, plantaris iv) lateral - peroneus brevis , peroneus longus Ankle Movements Plantarflexion Dorsiflexion Inversion Eversion General Ligament Sprains 1st, 2nd, 3rd degree Common Lower Leg & Ankle Injuries Inversion Ankle Sprain more common than eversion because of ligament and bony support stress is applied to the lateral side of the foot during plantar flexion and inversion most often injuring the Anterior Talofibular ligament (ATF) if stress is continued the Calcaneal Fibular Lig (CF) may be injured as well individual will report cracking or tearing sound at time of injury swelling and ecchymosis will be rapid and diffuse point tenderness over ATF may extend over CF Rx - PIER, modalities -horseshoe pad Should probably xray to rule out any possible fractures http://www.youtube.com/watch?v=SjprI020 XQ0&feature=related Eversion Ankle Sprain less common than lateral ankle sprains because of strong deltoid ligament, thus many are associated with fibular fractures mild to moderate pain with ankle eversion slower and less evident swelling point tenderness over deltoid ligament Rx – X-ray, PIER, modalities -horse shoe First Aid Care Immediately apply ice, compression and elevate Apply a horseshoe or doughnut pad, keep it in place with a elastic wrap. Have athlete rest , use crutches If needed refer to physician or hospital for x-rays . Syndesmotic ankle sprain AKA: high ankle sprain Approximately 10 – 15% of all ankle sprains involve the syndesmosis 30 % for collision sports ( football etc) MOI – almost always involves a direct blow to the lateral aspect of the leg with foot planted in external rotation s/s Min lateral swelling Possible med swelling Pain in anterolateral lower leg Point tenderness over the AITF lig , the interosseus membrane Pont tenderness over the ATF and possibly the sup ATF lig Disomfort /pain with DF ( AROM ) Loss of ankle function First Aid Care Immediately apply ice, compression and elevate Apply a horseshoe or doughnut pad, keep it in place with a elastic wrap. Have athlete rest , use crutches , may want to put in walking boot or cast for short period of time If needed refer to physician or hospital for xrays . Achilles Tendon Strain or Rupture probably the most severe acute muscular problem in lower leg 75% seen in males between 30 - 50 years mechanism of injury usually pushing off of the forefoot while knee is extending (racquet sports ) most ruptures occur 1 to 2 inches proximal to the distal attachments of the tendon on the calcaneus individual experiences sharp pain and hears or feels a POP in the tendon region - often described as a gun shot sound a common sensation is one of being hit in the back of the leg visible defect in the tendon inability to actively extend the foot (especially against resistance) swelling - bruising and a palpable defect in the tendon immediate referral to physician http://www.youtube.com/watch?v=AmDi08 rlR3I&feature=fvw First Aid Care Immediately apply ice, compression and elevate Immobilize the area in a splint or walking boot. Have athlete rest , use crutches Send to hospital or nearest medical facility. Achilles Tendinitis most common in lower leg tight heel cord – hyper-pronation repetitive heel running - a recent change in shoes or running surfaces - increase in distance or intensity pain present during and after activity increases with passive dorsiflexion and resisted plantar flexion point tenderness - diffuse or localized swelling aching or burning in the posterior heel occasionally fine crepitation can be palpated in the tendon with movement Rx - PIER, Modalities, NSAIDS-heel lifts reduced activity (rest) - especially running Lower Leg Contusion usually gastroc results in immediate pain and weakness and loss of function haemorrhage and muscle spasm quickly lead to a tender firm mass that is easily palpable ice on a mild stretch care must be taken for myositis ossificans Exercise Induced Compartment Syndrome 50-60% are anterior – characterised by exercise induced pain and swelling that is relieved by rest exercise induced aching leg pain and a sense of fullness, both over the involved compartment symptoms are almost always relieved with rest, usually with in 20 minutes exercise will produce swelling and tenderness to confirm a intra-compartmental pressure must be measured RX involves stretching and strengthening , PIER, and NSAIDS If symptoms persist , surgery is recommended Muscle Spasms and Cramps fatigue , loss of fluids or electrolyte, acute treated with ice , pressure and slow static stretch prevention - adequate water intake (electrolyte solution) regular stretching program Lower Leg Strain may be acute or chronic acute may be result of tearing followed by the inability to walk without pain point tenderness, swelling and muscle weakness will be present Rx - PIER, modalities, depends on severity Medial Tibial Stress Syndrome AKA : Shin splints Microscopic tears in the muscle attachment site on posterior medial border pain along the posterior-medial tibial border usually in the distal third Possible factors - excessive pronation , prolonged pronation , recent training changes (speed, form , running surface , distance) pain usually present at start of activity ,but decreases with activity only to return after activity, later stages pain present at all times may restrict activity RX - PIER, NSAIDS, (modalities) activity modification (rest) - low impact - non impact stretching and strengthening of intrinsic muscle of the foot Real key is to find cause …. http://www.youtube.com/watch?v=o5DXF VI6mTA&feature=related