Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
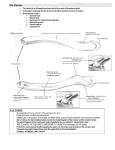
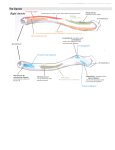
Acromioclavicular Separations: Etiology & Treatment By Jennifer R. Farrell A Senior Project April 11, 2001 Introduction • Acromioclavicular (AC) separation: – Acromion pulls apart from clavicle – Scapula falls away – Common in athletics – Classification varies Anatomy of the AC Joint • Diarthrodial joint. – Freely moveable. • Formed by the distal clavicle and acromion. • Coracoclavicular (CC), Acromioclavicular (AC) and Coracoacromial (CA) ligaments maintain joint reduction and stability. (Rockwood et al., 1998) Function of the AC Joint • Suspend upper extremity • Transmit forces to the axial skeleton. • Responsible for allowing arm to swing clear of the trunk (Hauser, 1996). • AC joint must have a strong ligament complex for support. Ligaments Involved • Acromioclavicular capsule – Four AC ligaments • Coracoclavicular ligament – Trapezoid and Conoid. • Coracoacromial ligament (Klassen, Morey & An, 1997) Motion of the AC joint • Elevate and abduct the arm. • The clavicle is capable of 30° to 40° of upward rotation (Field & Warren, 1996 and Hauser, 1996). • Motion occurs in a triaxial pattern (Klassen et al., 1997). • 90% of restraint to posterior displacement and resistance to horizontal translation by AC ligament (Field & Warren, 1996). • Coracoclavicular ligaments are the prime stabilizers and prevent superior dislocation (Klassen et al., 1997). Classification of Injury • AC joint injuries are classified based on the severity of injury sustained to the ligaments and supporting musculature (Rockwood, Williams & Young, 1998). • Traditionally only three types. • The most widely used 3-grade classification system is the Tossy system. Tossy System • Type I injury: – Basic sprain or contusion of the AC ligaments. – No tear or visible deformity, except slight swelling. • Type II injury: – Partial tear of the CC ligaments. – Superior clavicle, obvious swelling and difficulty lifting objects. • Type III injury: – Completely ruptured CC ligaments. – Severe pain, disability, swelling and marked deformity (Tossy, Mead & Sigmond, 1963). Classification of Injury • Since Tossy et al’s (1963) study, many studies have proposed expanding the classification system. • In addition, the Tossy system has been modified. Modifications to the Original Tossy System • Types I, II and III injuries modified in a study by Zlotsky, 1976. • Field and Warren (1996) divided types II and III into IIA & IIB, and IIIA & IIIB. Additions to the Tossy System • In a study by Gazielly (1995) types IV and V were proposed, while keeping the original Tossy classifications the same. • Hauser (1996) argued for six classes of AC separations while using the modified Tossy system proposed by Zlotsky (1976). Classification Overview • Most commonly used classification system presently (Rockwood et al., 1998). • Types I, II and III depict the modified Tossy system proposed by Zlotsky (1976). • Types IV, V and VI illustrate the classes proposed by Hauser (1996) and Gazielly (1995). (Rockwood et al., 1998) Mechanism of Injury Direct Mechanism* • * (Rockwood et al., 1998) Indirect Mechanism* Mechanics of Injury • With both direct and • There have been cases indirect trauma, the reported in which the clavicle usually detaches clavicle is lodged under from the acromion process the acromion, displaced superiorly. anterior, posterior or simply resting on top of • The clavicle will appear as the acromion.* a prominent protrusion on – *(Schwartz & Kuderna, 1988, the superior aspect of the Shildhaus & Meyers, 1987, & shoulder.* Leonard & Capen, 1983). – *(Irvin et al., 1998). Diagnosis of Injury • Weighted x-rays – bilateral • Basic anteroposterior and axillary views Treatment • Two types of treatments can be utilized to treat AC separations. – Conservative • Usually used for types I-III. – Surgical • Most often used for types III-VI. • Treatment options are controversial and highly debated. Conservative Treatment • Conservative treatment has been proven effective in grades I-III. – Gazielly (1995) found that surgery can be postponed for 2 to 3 months. • Conservative methods include: – – – – Taping/Strapping Ice/NSAIDs Modalities: E-Stim & Ultrasound Muscle strengthening Conservative Treatment • Basic strapping technique using a modified sling. • When taping, the same principle applies. • Generally it is best to support the arm as shown to limit stress placed on the AC joint.* * (Rockwood et al., 1998) Surgical Procedures • Four basic types of procedures used: – – – – Primary Acromioclavicular Joint Fixation Primary Coracoclavicular Ligament Fixation Excision of the Distal Clavicle Dynamic Muscle Transfer • With each of these procedures it is often necessary to remove devices used for reduction. Primary Acromioclavicular Joint Fixation • Most popular procedures used today (Rockwood et al., 1998). • Maintain reduction of the AC joint while the injured ligaments heal. • It is a common practice to repair damaged ligaments after joint fixation has occurred. Primary Acromioclavicular Joint Fixation • Pins, screws, suture wires and metal plates are used to bring the clavicle and acromion together. – Steinmann pins (Rockwood et al., 1998). – Wolter & Balser metal “crook” plates (Habernak, Weinstabl, Schmid & Fialka, 1993). Primary Coracoclavicular Ligament Fixation • Screws, ligament transfers, and synthetic & metal loops – Fix CC ligament – Suspend the clavicle from the coracoid process. • Examples include: – Bosworth screw (Bosworth, 1941). – GORE-TEX loop (Morrison & Lemos, 1995). – PDS bands (Hessman, Gotzen, Gehling & Ricter, 1995). Surgical Procedures • Examples of various surgical techniques (Rockwood et al., 1998). – A. Pins or screws across the joint. – B. Loops between the clavicle and coracoid. – C. A coracoclavicular lag screw. Excision of the Distal Clavicle • Origin unknown (Rockwood et al., 1998). • Usually done in conjunction with ligament transfer and fixation. – Weaver and Dunn (1972) • Treatment for chronic pain (Morrison & Lemos, 1995). Dynamic Muscle Transfer • Severely chronic cases. • Transfer of the trapezius and deltoid muscles. • Rarely used. • The actual procedure is not clear, and the findings vary (Rockwood et al., 1998) Complications • Conservative: – Calcification – Arthritis – Loss of strength – Removal of the device – Skin irritation • Surgical: – Wound infection – Migration of pins, screws, etc. – Scarring – Additional fractures – Excision due to wires – Removal of devices Rehabilitation Following Surgery • Limited motion • Sling for 1 to 2 weeks • Patients are to refrain from heavy lifting after removal of sling. • Muscle strengthening, and stretching at 6 weeks. • Modalities – E-Stim – Ultrasound • Rehabilitation can be more difficult and longer if devices must be removed (Habernek et al., 1993). Conclusion • Considerable disagreement in the literature regarding classification and treatment. • Type III remains the most controversial. • Various methods of treatment are available and administered with no standard. • Types IV, V and VI are rare. • Necessary to revert back to the initial Tossy system. Questions?