Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
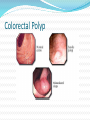
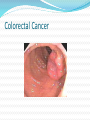
Sigid djuniawan,spB.FINACS Overview Classification of the causes of bleeding per rectum Evaluation of patient with bleeding per rectum Management of patient with bleeding per rectum OVERVIEW: The passage of blood per rectum is common symptom due to lesion of the distal small or large bowel. Fresh bleeding per rectum often presents as surgical emergency. The management involving: a. Resuscitation b. Determining the source of bleeding c. Controlling the bleeding The management is the combined effort of gasteroenterologist and surgeon with an emphasis on early intervention. THE CAUSES OF BLEEDING PER RECTUM According to the age According to the Site According to the age: (a) Rectal bleeding in children is due to: Meckel’s diverticulum Juvenile polyps Haemangioma Anal fissure Worms Rectal prolapse Intussusception (b) Rectal bleeding in adult is due to: Haemorrhoids Anal fissure Inflammatory bowel disease Meckel’s diverticulum Diverticulitis Angiodysplasia Aorto-intestinal fistula Ischemic colitis Neoplasm (Benign & Malignant) Coagulation disorder Chemotherapy According to the Site: Small bowel Large bowel The common causes of massive lower GI-Bleeding are: (a) Diverticular disease (b) Angiodysplasia (c) Aorto-enteric fistula The causes of bleeding per rectum are: (a) Haemorrhoids (b) Anal fissure (c) Large bowel cancer Surgical Pathology (Bleeding Per Rectum): Diverticular haemorrhage Angiodysplasia (Arteriovenous malformations) Meckel’s diverticulum Ischaemic bowel disease: (a) Acute infarctions (b) Ischaemic colitis Aorto-enteric fistula Surgical Pathology (Causes of bleeding per rectum): Internal haemorrhoids Anal fissure Large bowel cancer PATIENT WITH BLEEDING PER RECTUM History Clinical Examination Investigations History: Age of the patient Nature of haemorrhage: Colour Clots Drip with defecation Smear on paper Profuse loss Mixed with stool Perineal pain Abdominal pain Prolapse Diarrhoea Alteration in the bowel habit Abdominal distension Symptoms of anemia Miscellaneous symptoms: Weight loss Disturbance of micturation Family history Clinical Examination: General physical examination: - Anaemia, Weight loss, LN enlargement Abdominal Examination: - Abdominal mass, Distension Anorectal Examination: - Position of the patient left lateral with hips and knee flexed and the buttocks over the edge of examination couch. - Inspection - Patient straining - Palpation (Digital examination) - Proctoscopy - Sigmoidoscopy (Rigid) - F.O. Flexible sigmoidoscopy - Colonoscopy Special Investigations: CT Scan Selective angiography Isotope studies Barium enema Diagnostic laparoscopy / laparotomy MASSIVE BLEEDING PER RECTUM The principles of surgical management are similar to those for acute upper GI bleeding. Resuscitation Diagnosis of the cause Definitive surgical treatment Exclude upper GI source of bleeding Test for any bleeding diathesis Haemorrhoids The severity is graded by the degree of prolapse Grade 1 -no prolapse and cause painless bleeding. Grade 2 - prolapse on defecation, go back spontaneously. Seen on straining. Grade 3 - prolapse and have to be pushed back leading to bleeding and aching pain. Grade 4 - Can’t be pushed back leading to mucoid discharge, bleeding, pain, necrosis. Lack of soluble fiber and enough water in the diet, straining, and sitting longer than 2 minutes on the toilet which promotes prolapse of the anal cushions. Hemorrhoids may be inherited, but it may only be the behaviors and diet habits that are passed along. Failure to eat breakfast. Increase in abdominal pressure e.g. pregnancy, obesity, pelvic tumors, lifting, sitting, coughing, constipation, diarrhea, anal intercourse, aging. Correlation with decreased connective tissue strength as seen in hernias and genitourinary prolapse. Hemorrhoids can be exacerbated by excessive cleaning, rubbing, steroids, and hemorrhoid creams. Enlargement comes from the dragging of the hemorrhoids downward, weakened supporting tissue. Elevated sphincter tone increases straining. Risk Factors 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Past history of hemorrhoid symptoms or anal fissure Age 30-65 Heavy lifting, prolonged sitting Constipation/Diarrhea Pregnancy Failure to eat breakfeast. Diet-Spicy food, fats, alcohol, smoking, low water intake. Obesity Spinal cord injuries Increased sphincter tone Typical Hemorrhoid Symptoms Internal Hemorrhoids 1. chronic intermittent bright red bleeding with bowel movements. On tissue, in commode, or streaked on stool surface. 2. Feeling of fullness, swelling, extra tissue, incomplete BM. 3. Irritation or itching from seepage of mucus, fecal soiling or dermatitis from hemorrhoid creams causes rash. 4. Pain may occur with prolapse, associated external hemorrhoids or anal fissure. Visceral nerves above dentate line sense pressure not pain. External Hemorrhoids 1. Rectal pain from stimulation of 2. 3. 4. 5. somatic nerves of anal skin. Bulge of tissue on anal skin Blood on toilet tissue. Thrombosis leading to a hard painful lump. Skin tags left over after dilated external hemorrhoids, hemorrhoidectomy, or resolved thrombosis. Can trap stool and cause dermatitis and pruritus. History and Physical Name:_______________________ Date:_____________________________ Weight:______________________ BP:_______________________________ LOS:_________________________ Past RX:___________________________ CC:__________________________ Family Hx:_________________________ ROS:________________________________________________________________________ Bleeding:________________________ Pain:_______________________________ Irritation/Itching:__________________ Swelling:____________________________ Constipation:_____________________ Diarrhea:____________________________ Time on Commode:_________________ Straining:____________________________ OTC RX:__________________________ RX:_________________________________ Abdomen:______________________ Heart:____________________________ Fissure:_________________________ Sentinel Pile:_________________________ Ext Hem:__________________________________ Skin :___________________________ Int Hem: LL___ RA___ RP___ Spasm:_____________________________ Proctosigmoidoscopy;_________________________________________________________ Anoscopy:__________________________________________________________________ Anal Fissure Complete Rectal ProlapseProcidentia Anal Cancer Hypertrophic Anal Papillae Colorectal Polyp Rectal Villous Adenoma Colorectal Cancer Rectal Cancer Inflammatory Bowel Disease A. Dull mucosa and lack of normal vascular pattern. B. After Rx Crohn’s Disease Ulcerative Colitis Rectal Varices Rectal Hemangioma Radiation Proctitis Hemorrhoids or Not? Raise your level of suspicion 1. Recent changes in bowel habits, constipation, diarrhea, small caliber. 2. Abdominal Pain 3. Weight Loss 4. Anemia 5. Family history of Colo-rectal cancer 6. HIV infection, genital warts-HPV, rectal sex, cigarette smoking and increased risk of anal cancer 7. First-degree-only hemorrhoids. 8. Proctitis Bloody Stools-Lower GI Hemorrhage in Adults Melena-Black Tarry stools due to digested blood from upper digestive tract, esophagus, stomach, and jejunum. Esophagitis, varices, gastritis, gastric ulcer, peptic ulcer, angiodysplasia, jejunal diverticulum. Rarely from a slow bleeding right colon lesion. Black licorice, lead, iron, bismuth medicines-Pepto Bismol can also cause black stools. Hematochezia-Red or maroon-colored stools frequently foul smelling. Diverticulosis, angiodysplasia, inflammatory bowel disease, anorectal disease such as hemorrhoids, anal fissure, fistula in ano, colorectal polyps or cancer, ischemic colitis, infectious colitis, radiation enteritis, coagulopathy, aortoenteric fistula, post-polypectomy, post-hemorrhoidectomy, hemobilia, or massive UGI bleeding. Massive lower GI bleeding causes shock and may require transfusion. Diverticulosis is the most common cause of major lower GI bleeding. Blood mixed with stool, shorter duration of sx, and more episodes per month are more common with cancer, polyps, IBD when compared to hemorrhoids. Rectal Bleeding from Hemorrhoids or Anal Fissure-Blood on tissue, on outside of formed stool, or drips into commode after bowel movement. Blood is bright red in color. Typically mild and intermittent but occasionally massive. Hemorrhoids are the most common cause of chronic intermittent minor or non-massive lower GI bleeding associated with bowel movements. Hemorrhoid Procedures 1. 2. 3. 4. 5. 6. 7. 8. 9. Hemorrhoidectomy: Milligan-Morgan(open), Ferguson(closed). 1-2 days in hospital. Anesthesia required. Effective but more expense, pain, complications, and disability compared to office treatments. Its reputation causes many to avoid effective Rx and to buy ineffective hemorrhoid creams. PPH-Procedure for Prolapse and Hemorrhoids. Introduced in 1998. Lower pain than above but may have higher recurrence rate and similar complication rate. Learning curve. Perforations, stenosis, bleeding, or chronic pain may occur. Rubber Band Ligation causes ischemic necrosis and scarring, which results in shrinkage of tissue and fixation to rectal wall. Office procedure with minimal pain and complications. Low recurrence rate which can be Rx with rebanding. IRC-infrared coagulation requires 5-7 Rx, is more expensive than banding, higher recurrence rate, and may make external disease worse. Coagulates and scleroses tissue with heat. Less painful than old banders but more painful than CRH bander. Sclerotherapy-Phenol or vegetable oil, urea hydrochloride or hypertonic salt injected into base. Out of favor 2nd to complications and high recurrence rate. Bipolar diathermy-Coagulates and fibroses with heat. Direct-current electrotherapy-Coagulates and fibroses with heat. Doppler ligation-more expensive and no proven advantage over banding. Cryosurgery and anal stretch no longer recommended because of complications CRH Banding - by position Rubber Band Ligation Rectal Bleeding and Colonoscopy Bright red rectal bleeding with bowel movements is a common complaint. Benign lesions are the most common cause. 1. Incidence of Colon Cancer in patients with chronic intermittent rectal bleeding that is typical of hemorrhoids with no abdominal pain, change in bowel habits and rectal cancer not present on anoscopy is .8 - 3 %. In those under the age of 50 it is 0-3%. Other causes include polyps, fissures, diverticulosis, IBD. 2. The average approved reimbursement for colonoscopy is approximately $2200 compared to $1200 for banding. 3. Complications occur in 1-5% including perforation at a rate of .05-.3% and bleeding at a rate of .1-2%. 4. Colonoscopy misses 2-6% of colon cancers Do All Patients with Rectal Bleeding Typical of Hemorrhoids Need Colonoscopy Yes. Symptoms are unreliable and significant pathology is found in 20-40%; CRC, polyps, IBD, fissure, diverticulosis, angiodysplasia, rectal ulcers or proctitis, infectious or ischemic colitis. No. Having an effective office hemorrhoid treatment changes the approach. Banding the hemorrhoids first and restricting colonoscopy to those with positive FIT post banding is safe, cost effective, provides effective treatment, and avoids colonoscopy in over 90% of patients. Indications for Colonoscopy in Evaluation of Hemorrhoids 1. History or physical findings suggestive of cancer 2. 3. 4. 5. or IBD. Abdominal pain, weight loss, change in bowel habits, no obvious source of bleeding. Iron deficiency anemia Positive FIT/after RX Age over 40 with 1st degree relative with CRC or adenoma<60 and no BE or colonoscopy within 10 years. Age over 40 with two 1st degree relatives and no evaluation within 3-5 years. American Cancer Society Colorectal Cancer Screening Guidelines Beginning at age 50 (45 for African Americans), men and women who are at average risk for developing colorectal cancer should have 1 of the 5 screening options below: a fecal occult blood test (FOBT)* or fecal immunochemical test (iFOBT or FIT)* every year**, OR flexible sigmoidoscopy every 5 years, OR an FOBT* or FIT* every year plus flexible sigmoidoscopy every 5 years**, OR (Of these first 3 options, the combination of FOBT or FIT every year plus flexible sigmoidoscopy every 5 years is preferable.) double-contrast barium enema every 5 years**, OR colonoscopy every 10 years *For FOBT or FIT, the take-home multiple sample method should be used. **Colonoscopy should be done if the FOBT or FIT shows blood in the stool, if sigmoidoscopy results show a polyp, or if double-contrast barium enema studies show anything abnormal. If possible, polyps should be removed during the colonoscopy. CT Colonography 1. Helical CT scan creates two and three-dimensional images. Prepare with phospha-soda and bisacodyl. Air insufflation. 2. Accurate in detection of polyps greater than 10 mm and colon cancer. 3. False positives 15% unnecessary colonoscopy from retained stool, diverticular disease, thick or complex haustral folds, metal or motion artifacts. 4. May miss flat adenomas which are more aggressive. 5. Non therapeutic. 6. More expensive and not covered by insurance. Fissure Skin tags Skin tags are extra folds of skin around the anal verge. Caused by stretching of skin from dilated external hemorrhoids. May interfere with cleaning and add to pruritus ani. Cosmetic issue to some. Skin tag and can be removed or left alone depending on preference. Removal requires local anesthesia and office excision. Takes 15 minutes and leads to 2-3 days of discomfort. Associated skin tags