Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
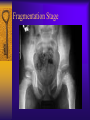
Legg Calve Perthes Disease Joseph Donnelly, M.D. December 10, 2001 Overview History Epidemiology/ Etiology Pathogenesis – Radiographic stages Presentation/ Exam Imaging Treatment History Late 19th century: “hip infections” that resolved without surgery First described in 1910 Early path studies: cartilaginous islands in the epiphysis Epidemiology Disorder of the hip in young children Usually ages 4-8yo As early as 2yo, as late as teens Boys:Girls= 4-5:1 Bilateral 10-12% No evidence of inheritance Etiology Unknown Past theories: infection, inflammation, trauma, congenital Most current theories involve vascular compromise – Sanches 1973: “second infarction theory” Etiology: blood supply Pathogenesis Histologic changes described by 1913 Secondary ossification center= covered by cartilage of 3 zones: – Superficial – Epiphyseal – Thin cartilage zone Capillaries penetrate thin zone from below Pathogenesis: cartilage zones Pathogenesis Epiphyseal cartilage in LCP disease: – Superficial zone is normal but thickened – Middle zone has 1)areas of extreme hypercellularity in clusters and 2)areas of loose fibrocartilaginous matrix Superficial and middle layers nourished by synovial fluid Deep layer relies on blood supply Pathogenesis Physeal plate: cleft formation, amorphis debris, blood extravasation Metaphyseal region: normal bone separated by cartilaginous matrix Epiphyseal changes can be seen also in greater trochanter, acetabulum Radiographic Stages Four Waldenstrom stages: – 1) Initial stage – 2) Fragmentation stage – 3) Reossification stage – 4) Healed stage Initial Stage Early radiographic signs: – Failure of femoral ossific nucleus to grow – Widening of medial joint space – “Crescent sign” – Irregular physeal plate – Blurry/ radiolucent metaphysis Initial Stage Initial Stage Fragmentation Stage Bony epiphysis begins to fragment Areas of increased lucency and density Evidence of repair aspects of disease Fragmentation Stage Fragmentation Stage Reossification Stage Normal bone density returns Alterations in shape of femoral head and neck evident Reossification Stage Reossification Stage Healed Stage Left with residual deformity from disease and repair process Differs from AVN following Fx or dislocation Presentation Often insidious onset of a limp C/O pain in groin, thigh, knee 17% relate trauma hx Can have an acute onset Physical Exam Decreased ROM, especially abduction and internal rotation Trendelenburg test often positive Adductor contracture Muscular atrophy of thigh/buttock/calf Limb length discrepency Imaging AP pelvis Frog leg lateral Key= view films sequentially over course of dz Arthrography MRI role undefined Differential Diagnosis Important to rule out infectious etiology (septic arthritis, toxic synovitis) Others: – – – – Chondrolysis JRA Osteomyelitis Lymphoma -Neoplasm -Sickle Cell -Traumatic AVN -Medication Radiographic Classifications Describe extent of epiphyseal disease Catterall classification= most commonly used – 4 groups based on amount of femoral head involvement – Also presence of sequestrum, metaphyseal rxn, subchondral fx Group I Group II Group III Group IV Lateral Pillar Classification 3 groups: – A) no lateral pillar involvment – B) >50% lat height intact – C) <50% lat height intact Salter-Thompson Classification Simplification of Catterall Based on status of lateral margin of capital femoral epiphysis Group A (Catterall I & II equivalent) Group B (Catterall III & IV equivalent) Prognosis 60% of kids do well without tx AGE is key prognostic factor: – <6yo= good outcome regardless of tx – 6-8yo= not always good results with just containment – >9yo= containment option is questionable, poorer prognosis, significant residual defect Prognosis Flat femoral head incongruent with acetabulum= worst prognosis Do not treat in reossification stage (>15mos) Non-operative Tx Improve ROM 1st Bracing: – Removable abduction orthosis – Pietrie casts – Hips abducted and internally rotated Wean from brace when improved x-ray healing signs Bracing Non-operative Tx Check serial radiographs – Q3-4 mos with ROM testing Continue bracing until: – Lateral column ossifies – Sclerotic areas in epiphysis gone Cast/brace uninvolved side Operative Tx If non-op tx cannot maintain containment Surgically ideal pt: – 6-9yo – Catterral II-III – Good ROM – <12mos sx – In collapsing phase Surgical Tx Surgical options: – Excise lat extruding head portion to stop hinging abduction – Acetabular (innominate) osteotomy to cover head – Varus femoral osteotomy – Arthrodesis Varus Osteotomy Late Effects of LCP Coxa magna Physeal arrest patterns Irregular head formation Osteochondritis dessicans The End