Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
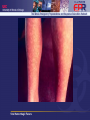
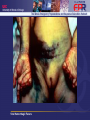
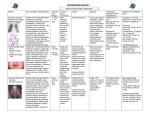
Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers Objectives • Describe the natural geographic distribution of VHF and scenarios suggestive of bioterrorism • Describe the clinical manifestations of VHF in general • List exposure classification of contact for cases of VHF • Describe infection control precautions for personnel caring for patients with VHF • List therapeutic options for patients with VHF Viral Hemorrhagic Fevers Case Presentation • 38 yo business man returned from West Africa via London, ill for 3 days – – – – – new onset fever chills severe sore throat diarrhea back pain • PE: T103.6 BP 90/60, alert – Skin with diffuse ecchymosis and a maculopapular rash on the extremities Viral Hemorrhagic Fevers MMWR 2004;53(38):891-897 Differential Diagnosis • Fever in a traveler – Malaria – Typhoid fever • Other Differential Diagnoses – – – – – Meningococcemia Rickettsial infection Leptospirosis Acute leukemia Idiopathic or thrombotic thrombocytopenic purpura Viral Hemorrhagic Fevers Hospital Course • Hospital Day #4 – Despite empiric antibiotics including antimalarials, pt develops acute respiratory distress syndrome (ARDS) – Required intubation Viral Hemorrhagic Fevers Differential Diagnosis • Fever in a traveler – Malaria – Typhoid fever – Yellow fever – Lassa fever Viral Hemorrhagic Fevers Hospital Course • Hospital Day #4 – Despite empiric antibiotics including antimalarials, pt develops ARDS – Required intubation • Hospital Day #5 – Local and state health departments notified – Investigational new drug (IND) protocol to administer IV ribavirin – Patient died before administration of any drug Viral Hemorrhagic Fevers Diagnosis • Clinical and post-mortem specimens sent to CDC • Lassa virus confirmed – Serum antigen detection – Immunohistochemical staining liver tissue – Virus isolation in cell culture – RT-PCR sequencing of virus Viral Hemorrhagic Fevers FAMILY/GEOGRAPHY AGENT CASE-FATALITY Filoviridae Sub-saharan Africa Ebola Marburg Arenaviridae West Africa (Lassa) South America, California (Whitewater) Old World: Lassa New World: Junin, Machupo, Guanarito Sabia, Whitewater arroyo Lassa:1-2% (up to 25% in hospitalized pts) Bunyaviridae Sub-saharan Africa Egypt, Yemen SW US (Hantavirus) Phlebovirus: Rift Valley Nairovirus: Crimean Congo Hantavirus: Sin Nombre Rift Valley: <1% overall 50% in hemorrhagic Flaviviridae Sub-saharan Africa Central Asia Yellow fever Dengue Omsk Kyasanur Viral Hemorrhagic Fevers 50-75% 25% 30% for New World Yellow Fever: 5-7% overall 50% in hemorrhagic www.cidrap.umn.edu/index.html accessed 2/4/05 Epidemiology • Incubation period – 2 days to 3 weeks for most VHF – Lassa fever: 21 days • Endemic regions – Sub-saharan Africa • Lassa fever causes 100-300,000 infections and 5,000 deaths each year • 20 imported cases reported worldwide • Human to human transmission has occured – South America Viral Hemorrhagic Fevers Why do VHFs make good Bioweapons? • • • • • • • Disseminate through aerosols Low infectious dose High morbidity and mortality Cause fear and panic in the public No effective vaccine Available and can be produced in large quantity Research on weaponization has been conducted Viral Hemorrhagic Fevers Clinical Presentation • Initial: – High grade fever, headache, myalgias, fatigue, abdominal pain • Advanced disease: – – – – – Bleeding Maculopapular rash Exudative Pharyngitis (Lassa) Meningoencephalitis Jaundice Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers Transmission • Direct contact with blood/body fluids/cadavers • Aerosol spray (droplet v. airborne) • Sexual transmission • Percutaneous • Bite of infected tick or mosquito Viral Hemorrhagic Fevers Infection Control • Lassa Fever in New Jersey Investigation: – 5 high risk contacts (wife, kids, visitor) – 183 low risk contacts • • • • 9 other family members 139 HCW at hospital: 42 labworkers, 32 RN, 11 MD 16 labworkers in Virginia and California 19 passengers on flight from London to Newark • No additional cases occurred Viral Hemorrhagic Fevers Infection Control Risk Category Description Surveillance Casual Contacts Remote contact with index case (eg, stayed in same hotel) VHF not spread by casual contact, no special surveillance Close Contacts More than casual (eg, Place under surveillance living with contact, once index case caretaker, shook confirmed hands with contact) High-Risk Contacts Mucous membrane Place under surveillance contact (eg, kissing, or as soon as consider penetrating injury diagnosis of VHF in involving contact with index case index case’s blood such as needlestick) CDC Update: Viral Hemorrhagic management Fevers of patients with suspected VHF-United States MMWR 1995;44:475-79 VHF Personal Protective Equipment • • • Airborne and Contact isolation for patients with respiratory symptoms – N-95 or PAPR mask – Negative pressure isolation – Gloves – Gown – Fitted eye protection and shoe covers if going to be exposed to splash body fluids Droplet and Contact isolation for patients without respiratory symptoms – Surgical mask – Gloves – Gown – Fitted eye protection and shoe covers if going to be exposed to splash body fluids Environmental surfaces – Cleaned with hospital approved disinfectant – Linen incinerated, autoclaved, double-bagged for wash Viral Hemorrhagic Fevers Treatment • Supportive care: – Fluid and electrolyte management – Hemodynamic monitoring – Ventilation and/or dialysis support – Steroids for adrenal crisis – Anticoagulants, IM injections, ASA, NSAIDS are contraindicated – Treat secondary bacterial infections Viral Hemorrhagic Fevers Treatment • Manage severe bleeding complications – – – – Cryoprecipitate (concentrated clotting factors) Platelets Fresh Frozen Plasma Heparin for DIC • Ribavirin in vitro activity vs. – – – – Lassa fever New World Hemorrhagic fevers Rift Valley Fever No evidence to support use in Filovirus or Flavivirus infections Viral Hemorrhagic Fevers Vaccination • Argentine and Bolivian HF – PASSIVE IMMUNIZATION • Treat with convalescent serum containing neutralizing antibody or immune globulin • Yellow Fever – ACTIVE IMMUNIZATION • Travelers to Africa and South America P. Jahrling, 29, Medical Aspects of Clinical and Biological Warfare; p591-602 ViralChapter Hemorrhagic Fevers This completes the current presentation. Viral Hemorrhagic Fevers