Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Germ theory of disease wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Gastroenteritis wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hepatitis B wikipedia , lookup
Common cold wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Neonatal infection wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Urinary tract infection wikipedia , lookup
Infection control wikipedia , lookup
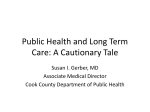
Klebsiella pneumoniae Presented by: Holly R. Wheeler Objectives Following this presentation the learner will be able to : Confirm the identification of Klebsiella pneumoniae based upon the results of the biochemical reactions, gram stain, colony morphology, and antigen classification. Relate K. pneumoniae to specific causes. Correlate K. pneumoniae with particular routes of transmission. Evaluate the symptoms associated with a K. pneumoniae infection. Assess diagnostic techniques for a K. pneumoniae infection. Evaluate who is most at risk for a K. pneumoniae infection and how the world has been affected. Evaluate the treatment options for a K. pneumoniae infection. Summarize preventative techniques taken against K. pneumoniae. Defining Characteristics Gram Stain: Gram negative rod. Biochemical Reactions: Oxidase: Negative Citrate: Positive Ferment inositol Hydrolyzes urea Do not produce ornithine decarboxylase Does not produce hydrogen sulfide Colony morphology: The presence of their polysaccharide capsule gives rise to large mucoid colonies on solid media. Antigen Classification: 8 O antigens and 77 K antigens and the virulence of all serotypes appears to be similar. There are no H antigens present because K. pneumoniae is non-motile. Media requirements: K. pneumoniae will grow on routine lab media (BAP, CHOC, and MAC). Citrate-containing media can be used to isolate this organism because this organism utilizes citrate has it’s sole carbon source. Gram Stain Being viewed at 100x Specific Causes • K. pneumoniae is considered to be apart normal enteric flora. • Considered to be pathogenic when it isolated from sterile sources especially body fluids. • Most commonly associated with nosocomial infections. • An international survey of K. pneumoniae bacteremia in critical care patients revealed that 43% of isolates produced extended spectrum β-lactamases (ESBLs). Although this rate may be lower in North America the possibility for an ESBL-producing organism must always be taken into consideration especially for all critical care patients. • K. pneumoniae has also been associated with Mycotic aneurysms of the internal carotid artery (ICA).* Routes of Transmission Hand carriage is generally regarded as the most common mode of transmission. K. pneumoniae has also been identified on environmental sources such as: blood pressure monitoring systems, ventricular traps, dialysate, ultrasonography coupling gel, and even hand disinfectant. K. pneumoniae has also been reported as being spread from newborn intensive care units to adult intensive care units; these reports have also been documented within international hospitals as well as domestic. K. pneumoniae is second only to Escherichia coli for nosocomial infections. Symptoms Symptoms from a K. pneumoniae infection can vary based upon the site of the infection. Symptoms from a pulmonary (pneumonia) infections can be: coughing, production of copious, thick purulent secretions and the formation of pulmonary abscesses. Appendicitis: abdominal pain, loss of appetite, nausea, vomiting, abdominal swelling, constipation, and fever. Pancreatic abscesses: a swollen and tender abdomen, nausea and vomiting, fever, a rapid pulse. Bacteremia: fever, chills, nausea, vomiting, and confusion. Cystitis (lower UTI): urinary frequency, fever, and flank pain. Pyeonephritis (upper UTI): fever, flank pain, and NO increased urinary frequency. Diagnosis Cultures for diagnosis can be obtained from blood, material from the trachea, ear canal, throat, and other external sites. Isolation can occur on routine lab media. Once K. pneumoniae has been isolated from the laboratory media it’s identification can be determined by biochemical testing. Biochemical testing can be conducted in test tubes, an API 20 strip or by the MicroScan. Modified Hodge Test (MHT) is a test that is conducted in the laboratory to detect carbapenemase production in isolates of the family Enterobacteriaceae. Of all the bacteria in the family Enterobacteriaceae Klebsiella pneumoniae carbapenemase (KPC) is the most commonly isolated. Countercurrent immunoelectrophoresis or a Quellung test can also be used to aide in the identification of K. pneumoniae. In situ hybridization techniques have been used to identify K. pneumoniae in phagocytes from blood specimens. Resistriction enzyme analysis and ribotyping of isolates have also been used to characterize the spread of more resistant strains. Prognosis Aggressive initial therapy directly correlates with survival. By limiting the duration of broadspectrum therapy greatly reduces the likelihood of drug resistant pathogens immerging; not only for the critical care patient but for the hospital and society as a whole. Numerous studies over the past two decades have demonstrated that that inadequate antimicrobial therapy leads to increased mortality, prolonged lengths of stay, and more undesirable outcomes. Survival rates can be decreased by 7.6% for every hour that treatment is delayed. Risk Factors Who is the most at risk? K. pneumoniae is commonly highlighted as a pathogen of debilitated adults and alcoholics. By 1985 nearly 50% of all reported Klebsiella outbreaks were in neonatal intensive care units. However, if any patient is immunocompromised in any way they are placed at a higher risk for contracting a K. pneumoniae infection. How has the world been affected? K. Pneumoniae infections are primarily opportunistic nosocomial infections but because this infection is so easily spread it has become international health risk as well. Treatment Drug of Choice: Fluoroquinolones: Levofloxacin (Levaquin) Moxifloxacin-oral (Avelox) Sulfamethoxazole/Trimethoprim (Bactrim, Septra). The treatment varies based upon the patients current treatment and their medical history. Example: Cancer patients infected with multiple strains have been treated successfully with a cephalosporin plus an aminoglycoside. Whereas patients infected with a single strain respond to treatment with a cephalosporin alone. Treatment (continued) Resistance: Klebsiella pneumoniae is characteristically resistant to Ampicillin. Plasma mid-mediated resistance to aminoglycosides also occurs commonly. Antimicrobial therapy has been made problematic due to certain strains emerging as ESBLs. ESBLs are widely distributed and their susceptibility patterns are dependant upon their regional differences. The outer-membrane of certain ESBLs have protein changes and porin changes that can create resistance to third-generation cephalosporins. There has also been significant correlation between Klebsiella ESBLs and ciprofloxacin resistance. Carbapenems, like Imipenem or Meropenem, are normally considered the agent of choice when treating a ESBL-producing Klebsiella pneumoniae. However, with Klebsiella pneumoniae carbapenemase (KPC)-producing organisms now emerging each isolate most be carefully and correctly identified so the patient can be treated quickly and effectively.* Prevention The best way to prevent a K. pneumoniae infection is using proper hand washing techniques. Sterilization of instrumentation that has direct patient contact can also aide against the spread of infection. Step 1: Apply soap to hands Step 2: Lather soap and wash for 15-30 seconds Step 3: Rinse hands under running water Epidemiology K. pneumoniae infections occur primarily as pathogens of the urinary tract, respiratory tract, biliary tract, bloodstream, and account for less than 10% of hospitalized cases of pneumonia in adults. A survey conducted by the Centers for Disease Control and Prevention (CDC) found that the nosocomial K. Pneumoniae infection rate was 16.7 infections per 10,000 patients discharged. References Klebsiella pneumoniae. [Photograph]. In Encyclopedia Britannica. Retrieved from http://www.britannica.com/EBchecked/media/100173/Gram-negative-bacilli-Klebsiellapneumoniae-isolated-from-a-lung-abscess CDC. (Photographer). (1976). Klebsiella pneumoniae 6689. [Photograph]. Atlanta, GA; CDC. Retrieved April 1, 2011 from http://phil.cdc.gov/phil/details.asp CDC. (Photographer). (1985). Klebsiella pneumoniae 6609. [Photograph]. Atlanta, GA; CDC. Retrieved April 1, 2011 from http://phil.cdc.gov/phil/details.asp The National Digestive Diseases Information Clearinghouse (NDDIC), Initials. (2008, November). Appendicitis. Retrieved from http://digestive.niddk.nih.gov/ddiseases/pubs/appendicitis/#symptoms The National Digestive Diseases Information Clearinghouse (NDDIC), Initials. (2008, July). Pancreatitis. Retrieved from http://digestive.niddk.nih.gov/ddiseases/pubs/pancreatitis/ O'Connell, JB, Darcy, S, & Reil, T. (2009). Extracranial internal carotid artery mycotic aneurysm: case report and review. Vascular & Endovascular Surgery, 43(4), Retrieved from http://ves.sagepub.com/content/43/4/410.full.pdf+html * Arnold, RS, Thom, KA, Sharma, S, Phillips, M, & Kristie Johnson, J. (2011). Emergence of klebsiella pneumoniae carbapenemase-producing bacteria. Southern Medical Journal, 104(1), Retrieved from http://ovidsp.tx.ovid.com.ahecproxy.ncahec.net/sp3.3.1a/ovidweb.cgi?&S=KGKIFPHNEGDDJGGINCCLAHIBPICIAA00&Complete+Referenc e=S.sh.16%7c1%7c1 References (continued) Fisher, B.G. (2009). Klebsiella. In R. Feigin, G. Demmler-Harrison, J. Cherry, & S. Kaplan (Eds.), Textbook of pediatric infectious diseases (pp. 1541-1545). Philadelphia, PA: Saunders Elsevier. Ahuja, D., Britt, B.B., Bryan, C.S. (2009). Selection of antibiotics in critical care. In B. Cunha (Ed.), Infectious diseases in critical care medicine (pp. 487-496). New York, NY: Informa Healthcare USA, Inc. Modified Hodge Test for Carbapenemase Detection in Enterobacteriacea. (n.d.) In Department of health and human resources centers for disease control and prevention. Retrieved from http://www.ndhealth.gov/microlab/Uploads/HodgeTest.pdf Smith, Kimberly (Photographer). (2004). Hand Washing Procedure Image 5739 [Photograph]. Atlanta, GA; CDC. Retrieved March 29, 2011, from http://phil.cdc.gov/phil/details.asp Smith, Kimberly (Photographer). (2004). Hand Washing Procedure Image 5740 [Photograph]. Atlanta, GA; CDC. Retrieved March 29, 2011, from http://phil.cdc.gov/phil/details.asp Smith, Kimberly (Photographer). (2004). Hand Washing Procedure Image 5744 [Photograph]. Atlanta, GA; CDC. Retrieved March 29, 2011, from http://phil.cdc.gov/phil/details.asp Buxton, Rebecca (Photographer). (2010). Fig 32 [Photograph]. Salt Lake City, Utah; University of Utah. Retrieved March 29, 2011, from http://microbelibrary.org/images/atlasmac/klebsiella%20pneumoniae%20fig32.jpg References (continued) Pneumonia Symptoms. (2006). Klebsiella pneumoniae. Retrieved from http://www.pneumoniasymptoms.org/klebsiella-pneumonia/klebsiella-pneumonia.html CDC. (2010, November 24). Klebsiella pneumoniae in healthcare settings. Retrieved from http://www.cdc.gov/HAI/organisms/klebsiella/klebsiella.html Leavitt, A Navon-Venezia, S, Chmelnitsky, I, Schwaber, M, & Carmeli, Y (2007). Emergence of KPC-2 and KPC-3 in Carbapenem-Resistant Klebsiella pneumoniae Strains in an Israeli Hospital. Antimicrobial Agents and Chemotherapy, 51(8). retrieved March 30, 2011, from http://aac.asm.org/cgi/content/full/51/8/3026 * Allen, M. (Photographer). (2005). Figure 32 klebsiella pneumoniae. [Photograph]. Retrieved from http://archive.microbelibrary.org/asmonly/details_print.asp?id=1976&Lang=&ISkip=20