Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
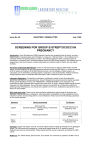
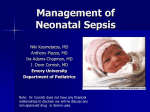
Neonatal sepsis Maria Victoria B. Pertubal, M.D. PGY1 I. II. III. IV. Definition of terms Epidemiology Etiology & Pathogenesis Evaluation and Diagnosis A. B. C. D. V. Clinical Manifestations Laboratory Management Algorithm of NB sepsis Treatment options Preventive management Definition of terms • Neonatal period – first month / 28 days of life • Neonatal sepsis –clinical syndrome in an infant 28 days of life or younger, manifested by systemic signs of infection and/or isolation of a bacterial pathogen from the blood stream Definition of terms • Early-onset vs. Late-onset sepsis Onset of symptoms 72 hours or ≥7 days of age Definition of terms • Intrapartum period • (NSVD) - from onset of labor / ROM to delivery • (CS) - between admission for labor and cord clamping How common is it and who are at risk? EPIDEMIOLOGY / RISK FACTORS • Overall incidence – 1-5 cases per 1000 live births • Preterm vs. Full term • GBS sepsis blacks>whites • asphyxia, meconium stained AF • Disrupted skin & mucosal integrity – (IV catheter) • Environmental exposure / direct contact Maternal RISK FACTORS • Socioeconomic – SE status, poor prenatal care, maternal substance abuse • Infectious : – Chorioamnionitis, fever (>38° C/100.4° F), venereal diseases, UTI/bacteriuria, GBS+ • Obstetrical: – amniocentesis, amnioinfusion, prolonged labor, PPROM, preterm labor Incidence of early- and late-onset invasive group B streptococcal (GBS) disease: Active Bacterial Core surveillance areas, 1990-2008*, and activities for prevention of GBS disease • • ACOG: American College of Obstetricians and Gynecologists; AAP: American Academy of Pediatrics. * Incidence rates for 2008 are preliminary because the live birth denominator has not been finalized. Reproduced from: Verani, JR, McGee, L, Schrag, SJ, et al. Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, 2010. MMWR Recomm Rep 2010; 59(RR-10):1. Original data from: Jordan, HT, Farley, MM, Craig, A, et al. Revisiting the need for vaccine prevention of late-onset neonatal group B streptococcal disease: a multistate, populationbased analysis. Pediatr Infect Dis J 2008; 27:1057. How is neonatal infection acquired? Routes of Infection Transplacental Vertical Horizontal Bacterial Viruses > Bacterial Bacterial >Viral (nosocomial/ Environmental) TORCHES GBS E. Coli HIV Coxsackie Polio Adenovirus EchoEnterovirus Varicella Parvovirus* TB Gonorrhea Listeria Anaerobes Malaria Lyme (maternal) Enterococcus Chlamydia Gonorrhea Ureaplasma Mycoplasma Syphilis Herpes HIV Hepatitis HPV Candida Klebsiella Staphylococcus –MRSA Pseudomonas Proteus Enterobacter Serratia C dificile Rotavirus Fungi Group B Streptococcus aka. Streptococcus agalactiae • Serotype distribution — corresponds to the capsular polysaccharide. – 9 serotypes: Ia, Ib, and II through VIII; serotype IX has been proposed • Serotypes Ia, Ib, II, III, and V account for more than 95 percent of early-onset cases in the United States and more than 90 percent of late-onset cases • Serotype III – meningitis; high proportion of late-onset infections • The distribution of serotypes and surface proteins among GBS isolates has important implications for the development of vaccines to prevent GBS disease. Pathways of ascending or intrapartum infection. (Figure 103-2 Nelson Pediatrics) Early onset sepsis is most commonly due to: A) Vertical / ascending transmission B) Horizontal transmission? How do we RECOGNIZE and DIAGNOSE sepsis? INITIAL SIGNS AND SYMPTOMS OF INFECTION IN NEWBORN INFANTS GENERAL Fever, temperature instability “Not doing well” Poor feeding Edema RESPIRATORY SYSTEM Apnea, dyspnea, Tachypnea, retractions, Flaring, grunting, Cyanosis CARDIOVASCULAR SYSTEM Pallor; mottling; cold, clammy skin Tachycardia Hypotension Bradycardia RENAL SYSTEM Oliguria GASTROINTESTINAL SYSTEM Abdominal distention Vomiting, Diarrhea, Hepatomegaly HEMATOLOGIC SYSTEM Jaundice, Splenomegaly, Pallor, Petechiae, purpura, Bleeding CENTRAL NERVOUS SYSTEM Irritability, lethargy, Tremors, seizures, Hyporeflexia, hypotonia, Abnormal Moro reflex, Irregular respirations, Full fontanel, Highpitched cry Kliegman: Nelson Textbook of Pediatrics, 19th ed. Copyright © 2011 Saunders, An Imprint of Elsevier History • Review of the pregnancy, labor, and delivery – Duration – Mode of delivery – Newborn condition at delivery (APGAR & BW) Maternal-Neonatal Risk factors for sepsis • • • • • Intrapartum maternal temperature ≥38ºC (100.4ºF) Delivery at <37 weeks gestation Chorioamnionitis Five minute Apgar score ≤6 Evidence of fetal distress Membrane rupture ≥18 hours – risk of proven sepsis increases 10 fold to 1 % • Maternal GBS colonization – Use of Intrapartum antibiotic prophylaxis (IAP) differential diagnosis • • • • other systemic bacterial infections, neonatal hypoxia, in-born errors of metabolism, neonatal respiratory distress. What LABORATORY exams will you request? Laboratory BLOOD TESTS: • Blood culture establishes a definitive diagnosis • Other blood tests: – CBC – within 24h – Immature to total PMN ratio (I:T ratio) • Inflammatory markers: – CRP, cytokines, procalcitonin (released by parenchymal cells in response to bacterial toxins Laboratory Urine : • Culture – for all infants older than 3 days of age – If done on younger infants, it may only reflect high grade bacteremia rather than isolated UTI Other ancillary • Chest X-ray – If with clinical signs of RDS • Cultures from other potential foci of infection – Secretions/pus Laboratory BLOOD TESTS: • Blood culture establishes a definitive diagnosis • Other blood tests: – CBC – within 24h – Immature to total PMN ratio (I:T ratio) • Inflammatory markers: – CRP, cytokines, procalcitonin (released by parenchymal cells in response to bacterial toxins Laboratory CSF analysis: • should be considered in all neonates; clinical signs of meningitis can be lacking in young infants • Send for : – Culture – gram stain, – cell count – protein – glucose Bacterial meningitis CSF findings Culture Gram stain WBC protein glucose Can be negative in 30-38% of 20 percent of neonates with cultureconfirmed bacterial meningitis have negative >20 to 30 cells/ microL preterm >150 mg/dL preterm <20 mg/dL Gram-stained (1.1 mmol/L) >1000 *greater count in Gneg meningitis term >100 mg/dL in term <30 mg/dL (1.7 mmol/L) What is our Management GOAL? Be HIGHLY suspicious of all potential neonatal sepsis cases Algorithm for secondary prevention of early-onset group B streptococcal (GBS) disease among newborns •Full diagnostic evaluation : blood culture, complete blood count (CBC) w/ differential and platelet counts, chest radiograph (if respiratory abnormalities are present), lumbar puncture (if patient is stable enough to tolerate procedure and sepsis is suspected). † Antibiotic therapy - directed toward the most common causes of neonatal sepsis, intravenous ampicillin for GBS and coverage for other organisms (including Escherichia coli and other gram-negative pathogens) -must take into account local antibiotic resistance patterns. § Consultation with obstetric providers is important to determine the level of clinical suspicion for chorioamnionitis. Chorioamnionitis is diagnosed clinically and some of the signs are nonspecific. ¶ Limited evaluation blood culture (at birth) CBC with differential and platelets (at birth and/or at 6–12 hours of life). ** See indications for intrapartum GBS prophylaxis. †† If signs of sepsis develop: Conduct full diagnostic evaluation Initiate antibiotic therapy §§ observation may occur at home If ≥37 weeks’ gestation, after 24 hours if other discharge criteria have been met access to medical care is readily available, person who is able to comply fully for home instruction will be present. If any of these conditions is not met, the infant should be observed in the hospital for at least 48 hours and until discharge criteria are achieved. For LOW RISK ¶¶ Some experts recommend a CBC with differential and platelets at age 6–12 hours. ¶ Limited evaluation blood culture (at birth) CBC with differential and platelets (at birth and/or at 6–12 hours of life). What is the value of antenatal screening for GBS? Year 2002 • Universal screening at 35--37 weeks' gestation for maternal GBS colonization and use of intrapartum antibiotic prophylaxis has resulted in substantial reductions in the burden of early-onset GBS disease among newborns. Incidence of early- and late-onset invasive group B streptococcal (GBS) disease: Active Bacterial Core surveillance areas, 1990-2008*, and activities for prevention of GBS disease • • ACOG: American College of Obstetricians and Gynecologists; AAP: American Academy of Pediatrics. * Incidence rates for 2008 are preliminary because the live birth denominator has not been finalized. Reproduced from: Verani, JR, McGee, L, Schrag, SJ, et al. Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, 2010. MMWR Recomm Rep 2010; 59(RR-10):1. Original data from: Jordan, HT, Farley, MM, Craig, A, et al. Revisiting the need for vaccine prevention of late-onset neonatal group B streptococcal disease: a multistate, populationbased analysis. Pediatr Infect Dis J 2008; 27:1057. Recommended regimens for intrapartum antibiotic prophylaxis for prevention of early-onset group B streptococcal (GBS) disease* Algorithm for screening for GBS colonization and use of intrapartum prophylaxis for women with preterm* labor (PTL) SUMMARY • Neonatal sepsis is is classified by the infant's age into early-onset sepsis (≤3 to 7 days) and late-onset sepsis (>3 or 7 to 28 days). • Group B Streptococcus (GBS) and Escherichia coli are the most common bacteria causing neonatal sepsis • Risk factors for neonatal sepsis in term and late preterm infants include intrapartum maternal temperature ≥38ºC (100.4ºF), chorioamnionitis, five minute Apgar score ≤6, maternal GBS colonization, and membrane rupture ≥18 hours. SUMMARY • Evaluation include a prenatal history, delivery, complete physical examination, and a laboratory evaluation that minimally includes a blood culture. • overall incidence of early onset GBS disease in NB substantially decreased over the last decade with universal screening for maternal GBS and use of IAP • Initial empirical antibiotic therapy for suspected GBS disease should include broad coverage for the most likely pathogens (Ampicillin/Vancomycin-Gentamicin/Cefotaxime) any deviation from an infant's usual pattern of activity or feeding should be regarded as a possible indication of systemic bacterial infection Nizet, V, Klein, JO. Bacterial sepsis and meningitis. In: Infectious diseases of the Fetus and Newborn Infant, 7th ed, Remington JS et al (Ed), Elsevier Saunders, Philadelphia 2010. p.222. SUMMARY Routine hand hygiene by health care professionals is the best way to prevent health care-associated spread of GBS infection Salamat po