Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
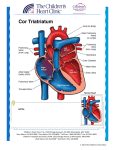
Case presentation Maram Mobara Najla is a 26y old girl Saudi, from riyadh . Single Known to have B-thalassaemia major based on Hx and Hb electrophorresis findings Admitted through ER with dyspnea + fever For 3 days HPI : dyspnea+fever for 3days patient was in her usual state of health when she developed progressive dyspnea that started with mild exertion (usual state) and became marked even during rest over 3 days It was associated with mild-moderate dry cough. No Hx of hemoptysis Pateint gave Hx of increased body temp. for 3 days before presentation associated with sweating. No chills/rigors. Documented in ER. No Hx of chest pain. Hx of palpitation with illness but of no specific character and not followed by syncope. Hx of LL edema Hx of abdominal distention for years Hx of mild truama induced epistaxis About her chronic illness; known to have thalassaemia since she was 6m age. S/P spleenectomy at age of 10 y. Since that time she is on multiple transfusion Tx , average 2 PRBC every 50 days, Last blood transfusion was 1m before presentation at KFMC. Was on SC dessferal , not complient for whole last year. F/O RKH,KFMC. Systemic review GIS: chronic abdominal distention, jaundice for long time, mild on & off heartburn associated with food, no recent change in bowel habits (12times/day), no hx of nausea or vomiting. Renal: no hx of increase in freq, dysuria, change in colour. no Hx of polyuria, polydypsia no Hx of heat intolerance, no hx of skin pigmentation. Poor weight gain Primary amenorrhea. Hx of progressive generalized boneaches, limitation of movement, proximal weakness over last 5m, no hx of joint swelling or change in colour. No hx of headache, syncope, vertigo, seizures or numbness PMH No other causes for hospital admission No known allergies Family hx : parents are separated No similar illness in the family ? Social: intermediate school Poor socioeconomic status. 5 2 5 2 In the ER: she was febrile 38.5 signs of Rt side HF CXR marked cardiomegaly ECG: sinus rhythem rate:100/min axis: about 90 pifid p wave, PR interval 0.2 RSR pattern in V1,2 Bedside echo: Rt side dilatation, tricuspid regurgitation Hb 8.3 , received 1 PRBC Hb:10.2 In the ward Looks ill, cyanotic, pale and jaundiced In mild-moderate respiratory distress , O2 2L/min via NC , O2 sat:93-95%, RR: 24/min Very small body built, much younger than stated age, tanner stage 2 Frontal bossing, no clubbing No evidence of LNP, thyroid gland impalpable JVP: 8cm above AOL VS: temp. low grade fever PR: 90/min regular, BL.P: 110/60 mmHg Chest: chest deformity. fair airentery, Bi equal vesicular breathing, inspiratory crepitation up to middle zone. No wheezes. Normal percussion note CVS: left parasternal heave, palpable 2nd heart sound S1+ loudS2(P2) Pansystolic murmer allover auscultation areas more in tricuspid area Abdomen: marked abdominal distension Visible lower liver border Not tender, 8cm palpable liver below CM, LS: 14 cm. MSS: waisting muscles of upper& lower limbs, mild generalized bony tenderness. CNS: normal higher center functions face symmetrical with normal CNx examination patient can’t raise hand above head, difficult standing normal symmetrical tone and reflexes power 3/5 generally, 2/5 at shoulder and hip joints normal sensation Differential Diagnosis Investigations CBC: HB 8.6 10.4 8.3 WBC10.45 102 (nucleated RBC) RBC3.2 MCV89 MCH28 Ret.12.72 U&E Random BS 3.9 UA 9.5 74 Htc29.4 RDW18.5 PLT224 LFT: T.bilirubin 22 direct 11 albumin 27 Alanine AT 52 Aspartate AT 141(4) GGT 360 (6) globulin 50 (40) coagulation profile Viral screening Iron 47 , ferritin 13627 Bone profile Ca corrected 1.88 2.29 inorganic phosphorus 1.69 ALP 279 PTH 7.44 TFT FT4 10.5 TSH 18.9 FSH 0.39 LH 0.65 estradiol 43.63 prolactin 231 Departmental echo Rt heart dilatation , Lt atrial too RVSP 115 TR significant Atrial Septal Defect Abdominal US homogenous marked hepatomegly no gall bldder inflammatory changes normal kidneys 3 early morning blood C/S 7 days Urine culture result negative Sputum positive for MRSA Hospital course improved with course of IV lasix then shifted to oral . Sating well in RA Low grade fever IV ceftriaxone , IV vancomycin 2 days temp. 37 max Hematology team complicated iron transfusion tx Chelation Tx dessferal pump machine Cardiology team case of ASD , eisenmenger syndrome most likely fixed PHT trial of low dose nifidipine case of low grade fever although on IV Ab, to role out IE T/F blood culture TEE to role out vegitation Pulmonary HTN Definition : mean pulmonary artery p. > 25 mmHg at rest or 30 mmHg with exercise, as measured by right heart catheterization classification Pulmonary arterial hypertension (PAH) Idiopathic (IPAH) Familial (FPAH) Associated with : Collagen vascular disease Congenital systemic-to-pulmonary Pulmonary hypertension with left heart disease Pulmonary hypertension associated with lung diseases and/or hypoxemia Pulmonary hypertension due to chronic thrombotic and/or embolic disease Miscellaneous Intracardiac shunt PAH caused by pulmonary blood volume overload. (ASD) is the most common congenital lesion in adults after bicuspid aortic valve. ASD often asymptomatic until adulthood, The normal pulmonary vasculature accommodates the increased volume of flow in patients with an ASD by recruitment of previously unperfused vessels. PA pressures rise significantly if volume of pulmonary blood flow exceeds 2.5 times baseline. related to the degree and duration of right heart volume overload Here where patient develop Eisenmmenger syndrome Dilated cardiomyopathy HF and dilated cardiomyopathy are common causes of PHT. study of 108 patients with dilated cardiomyopathy, 26 % had a pulmonary artery systolic pressure above 40 mmHg, as determined by echocardiography Mangment of PHT Early identification and treatment Prior to the initiation of therapy, the severity of the PH should be determined. (response assessment) Primary therapy underlying cause of the PH anticoagulant therapy to patients with IPAHT (sporadic or familial), or who have a high risk for thromboembolism diuretics be given if fluid retention is present supplemental O2 for patients with group 3 PH / resting or exercise hypoxemia Advanced therapy Principle : Abnormal vasoreactivity and cell proliferation characterize PH. This is best established among patients with group 1 PAH, but is probably true for patients with group 2, 3, &group 4. Most pharmacologic agents used to treat PH promote vasodilation and are antiproliferative. These include prostanoids (eg, epoprostenol, treprostinil, and iloprost), endothelin receptor antagonists (eg, bosentan), and phosphodiesterase-5 (PDE5) inhibitors (eg, sildenafil). Calcium channel blockers (nifedipine) are also used but have limited benefit as they are pure vasodilators without antiproliferative effects prostanoids (eg, epoprostenol, treprostinil, and iloprost), endothelin receptor antagonists (eg, bosentan) phosphodiesterase-5 (PDE5) inhibitors (eg, sildenafil). Calcium channel blockers (nifedipine) are also used but have limited benefit as they are pure vasodilators without antiproliferative effects Vasoreactivity test administration of a short-acting vasodilator, right heart catheter. Agents commonly used include epoprostenol, adenosine, and inhaled nitric oxide positive if mean pulmonary artery pressure decreases at least 10 mmHg and to a value less than 40 mmHg, with an increased or unchanged cardiac output, and minimally reduced or unchanged systemic BP. Ca channel blockers achieve prolonged survival sustained functional and hemodynamic improvement observational study of 64 patients with IPAH that compared vasoreactive patients who received CCB therapy versus a combination group that included patients who were not vasoreactive ,None received CCB therapy. Five year survival was greater among patients who received CCB therapy (94 versus 55 percent) This evidence is limited by the absence of randomized trials comparing CCB therapy versus no therapy in vasoreactive patients only initiated with nifedipine (30 mg/day) or diltiazem (120 mg/day), then increased to the maximal tolerated dose . Systemic blood pressure, heart rate, and oxygen saturation should be carefully monitored during titration. Epoprostenol It improves hemodynamic parameters, functional capacity, and survival in patients with IPAH a trial that randomly assigned 81 patients severe (ie, NYHA class III or IV) IPAH intravenous epoprostenol versus standard therapy for 12 weeks . Intravenous epoprostenol improved quality of life, mean pulmonary arterial pressure ( -8 versus +3 percent), pulmonary vascular resistance (-21 versus +9 percent), and exercise capacity, as measured by a six minute walk test (+47 versus -66 meters). Eight patients died during the trial, all of whom were in the standard therapy group. Pulmonary Hypertension and bThalassemia Major:Report of a Case, Its Treatment, and a Review of the Literature Tam and Farber.et,al.Amer J of Hema.81:443– 447 (2006) Case report A 28-year-old man with b-thalassemia major Splenectomy , hepatitis C, diabetes, and hemosiderosis Presented with a 3-month history of worsening dyspnea on exertion Oxygen saturation with minimal exertion (40 steps) on room air was 68 to 86%. Elevated jugular venous pressure Clear lungs, pulmonic tap Systolic ejection murmur, right ventricular heave, and Pulsatile liver. Hematocrit of 26% and ferritin was 14,000 mg/L. TEE showed right atrial dilation, right ventricular hypokinesis and dilation, severe tricuspid regurgitation, and estimated right ventricular systolic pressure of 78 mm Hg. High resolution CT scan of the chest no interstitial lung disease and ventilationperfusion scan was normal. Pulmonary function testing : normal spirometry and lung volumes with decreased diffusion capacity. Serologic markers for connective tissue disease and HIV were negative. Cardiac catheterization confirmed the diagnosis of pulmonary hypertension; mean pulmonary arterial pressure was 47 mm Hg. Liver biopsy demonstrated 4þ/4þ hemosiderosis with micronodular cirrhosis; comparison Female 26 years Iron overload: ferritin 13,627 Signs of Rt HF echo: Rt atrial, ventricular dilatation, left atrial dilatation, TR, Rt vent P.of 112, ASD Male 28 years Iron overload: ferritin 14000 Signs of Rt HF echo Rt atrial & ventricular dilation, severe TR, Rt ventricular P. of 78 mm Hg CT chest: PFT CT chest: no interstitial lung disease & ventilation-perfusion scan was normal. PFT: normal spirometry and lung volumes with decreased diffusion capacity Cardiac catheterization confirmed the diagnosis of PHT Liver biopsy demonstrated hemosiderosis with micronodular cirrhosis Continuous intravenous epoprostenol, titrated to a dose of 12 ng/kg/min, in addition to daily 12-h intravenous infusion of desferoxamine(3g) After 8 weeks of therapy, oxygen saturation with ambulation on level ground was 97% on room air. After 5 years of continuous epoprostenol, during which time the dosage had been increased to 22 ng/kg/min based on symptoms and clinical status, the patient could climb five flights of stairs while maintaing O2 95% Repeat right heart catheterization after 4 years of treatment demonstrated a mean Pulmonary A.P. of 33 mm Hg Of note, the ferritin level decreased to 12,000 mg/L and 1700 mg/L at 8 weeks and 5 years of therapy, respectively. fewer blood transfusions were given during this 5-year period. Comments