Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
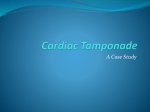
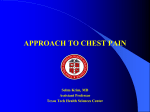
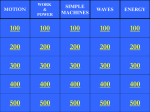
Obstructive shock implies there is an obstruction to blood flow. This means treatment requires alleviation of the obstruction. Therefore, this type of shock needs to be clearly and early identified so the correct treatment can be applied. If an arrest occurs in the patient with obstructive shock, CPR and associated ACLS strategies will not be effective because there is an obstruction to flow. Additionally, the mechanical complications of ventricular septal rupture and papillary muscle rupture represent surgical emergencies and thus must be immediately identified. Tension Pneumothorax Cardiac Tamponade Aortic Dissection Pulmonary Embolus This module will focus on patient risk factors and nursing assessment and recognition. Who is at risk? Blunt trauma Positive pressure mechanical ventilation PEEP Underlying pulmonary disease Clamped or clotted water seal drainage system (chest tube) Airtight dressing on open pneumothorax Accumulation of air into the pleural space without a means of escape causes complete lung collapse and potential mediastinal shift. Emergency decompression or a chest tube is required. Chest pain Dyspnea, cough Tachycardia Asymmetrical chest excursion Diminished to absent breath sounds on affected side › Dramatic increases in peak inspiratory pressures on a mechanical ventilator Early › › › › › If mediastinal shift: › Tracheal shift away from affected side Late › JVD › Hypotension Note: Tension pneumothorax can be diagnosed with bedside assessment. When a patient becomes hypotensive after being put on positive pressure mechanical ventilation – always consider tension pneumothorax as a possible cause. Other possible causes of hypotension after positive pressure mechanical ventilation include: › Volume depletion › Development of auto PEEP (patient needs a longer expiratory time) Who is at risk: Post CABG Post myocardial infarction – free wall rupture o Post ablation / post pacemaker o Malignancy / S/P radiation therapy o Infection resulting in pericarditis o Anyone with known pericardial effusion o Trauma o o Clinical syndrome caused by accumulation of fluid in the pericardial space. Results in reduction in ventricular filling and ultimately hemodynamic compromise. › The right ventricle cannot relax and fill. Tamponade must be identified because it requires treatment with pericardiocentesis or surgical pericardial window. 10 Patient feeling of impending doom Pulses alternans or electrical alternans Beck’s Triad Hypotension, Distended neck veins, Muffled heart sounds Pulses paradoxus Equalization of filling pressures if a PA catheter is present (RAP, PAD, PAOP within 5mm of each other) An echocardiogram will provide a definitive diagnosis. 11 To measure the pulsus paradoxus, patients are often placed in a semirecumbent position; respirations should be normal. The blood pressure cuff is inflated to at least 20 mm Hg above the systolic pressure and slowly deflated until the first Korotkoff sounds are heard only during expiration. At this pressure reading, if the cuff is not further deflated and a pulsus paradoxus is present, the first Korotkoff sound is not audible during inspiration. As the cuff is further deflated, the point at which the first Korotkoff sound is audible during both inspiration and expiration is recorded. If the difference between the first and second measurement is greater than 12 mm Hg, an abnormal pulsus paradoxus is present. (Yarlagadda, Chakri, 2005 Cardiac Tamponade. Retrieved 3-22-06 from www.emedicine.com) 15 Who is at risk? Hypertension is present in most patients with dissections Congenital disorders affecting connective tissue such as Marfan Syndrome or Ehlers-Danlos syndrome; also presence of bicuspid aortic valve After procedures where aorta or the aortic branches have been Note: A retrograde cannulated. aortic dissection can also cause a myocardial infarction. A Tear in the Intima of the Aorta – Allows Blood in the False Channel Blood in the False Channel can Obstruct Flow in the True Lumen Chest or back pain often described as ripping or tearing. Variation in upper extremity blood pressure > 20 mmHg. Pulse deficit. Focal neurological change. New murmur of aortic regurgitation. Timing: Begins early in diastole Location: 3rd intercostal space LSB Radiation: Toward apex Configuration: Decrescendo Pitch: High Quality: Blowing 20 What are the Risk Factors? Stasis of blood Prolonged immobilization after surgical procedures Venous obstruction Heart failure Shock / Hypovolemia Varicose veins Obesity Hypercoagulability Polycythemia vera Sickle cell disease Malignancy Recent trauma Injury to the vascular endothelium Central venous and arterial catheters Phlebitis Significance of PE Death within 1 month of diagnosis: › 12% of PE cases PE cause of death in 10% of hospitalized patients PE from DVT is leading cause of preventable hospital mortality › 20% of untreated proximal DVT will result in PE › 10-20% of these PE will be fatal › Anticoagulation decreases mortality 5 to 10 fold 22 Massive PE results in an obstruction to blood flow. Large to massive when 50% of pulmonary artery bed is occluded Medium-sized emboli › Dyspnea › Substernal chest › Impending doom › Hypoxemia › Syncope › Sign and symptoms of right heart strain or right-ventricular failure › Signs of right-ventricular strain on ECG. › Sudden shock. › Pulseless electrical activity. › › › › › › discomfort/pleuritic chest pain Many non-specific signs Tachypnea Tachycarida Rales Accentuated 2nd heart sound Respiratory alkalosis 24 • • • Transient ECG changes T wave inversion (or other ECG signs of ischemia, injury, infarction) in both inferior and anteroseptal leads Elevated ST segments aVR and V1-V2 Signs of Right Heart Strain • ST or atrial tachycardia (or fib / flutter) • Prominent S waves in I and aVL • Deep S wave in Lead I (S1); and Q wave/inverted T in Lead III (Q3/T3) • RAD or incomplete or complete RBBB • Widespread S waves • Prominent P waves in inferior leads (right atrial strain) 25 Note the T wave inversion in the limb leads and precordial leads. Also - big P waves in II, III, and aVF. 26 Incidence › 10% MI deaths Definition › Myocardial leakage from free wall – hemipericardium – Tamponade › Perceived sudden; often slow tear Associated Factors : Delayed presentation to the Septal involvement = VSD Posterior wall = Risk for papillary muscle hospital 27 Free wall rupture. Post-infarction regional pericarditis precedes rupture (94% of the time) T Wave Patterns in Post-infarction Regional Pericarditis Persistently positive T waves 48 hours after an MI ST segment reelevation Premature reversal of T wave inversion to positive 29 If myocardial rupture involves the free wall it will result in cardiac tamponade. › We have already reviewed the signs and symptoms of cardiac tamponade. The next two slides show a patient with anterior wall MI . In the second slide – note that the T waves in lead V3 have failed to invert 48 hours after admission. The patient developed cardiac tamponade and went to OR for a cardiac window. Timing: Continuous Location: 3-4 LSB Radiation: Widely throughout the precordium Configuration: Plateau Pitch: High Quality: Harsh 33 34 35 Timing: Holosystolic Location: Mitral area Radiation: To the left axilla Configuration: Plateau Pitch: High Quality: Blowing, harsh or musical Acute papillary muscle rupture will identified by a new murmur of mitral regurgitation and by the presence of new onset pulmonary edema. 36 37 There are many reasons for hypotension. However, when hypotension is not easily corrected by interventions such as volume administration, it is important to rule out obstructive shock. Remember: Obstructive shock requires interventions beyond BCLS and ACLS and thus must be identified early. 38 Tamponade Tension Pneumothorax Pulmonary Embolus › › › › › › › › › › › › › Risk factors (trauma, post OHS / procedure, large MI – late presentation) Beck’s triad Pulses Paradoxus Pulses / Electrical Alternans Risk factors (Conversion to PPV, existing chest tube, trauma) Lung sounds Hypotension JVD Mediastinal shift (very late sign) Risk factors (Virchow’s triad) Tachypnea (most common sign) Respiratory Alkalosis ECG signs Right axis deviation RBBB Tall P waves inferior leads T wave inversion (limb and precordial leads) Prominent S waves 1 and aVL Deep S wave in Lead I (S1); and Q wave/inverted T in Lead III (Q3/T3) › ST / New atrial arrhythmia 39 Acute Aortic Dissection › Risk factors (HTN most common) › Tearing or ripping description of CP or back pain › Diastolic murmur of Aortic regurgitation › Bilateral arm BP variation › Pulse deficit › Focal neurological deficit › Co-existing Inferior MI Mechanical Complications of MI › Warning signs – regional pericarditis (failure of T wave to invert within 48 hours, premature reversal of T wave inversion, Re-elevation of ST segments) › Papillary Muscle Rupture Holosystolic murmur Acute pulmonary edema › VSD Continuous murmur Please reflect on a patient you have cared for with one of the emergency situations discussed in this module. Describe any assessment findings you observed in this patient and your response to these signs and symptoms. Please identify one new concept you learned during this module. Please identify one change in clinical practice you will make based on what you have learned in this module. Thank You. Please add to your portfolio a clinical example where your patient assessment resulted in change in patient care or outcomes. Note: This does not need to be in a patient with obstructive shock.