Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
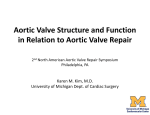
Corso Integrato di medicina d’urgenza, terapia intensiva e infermieristica clinica applicata Lezioni di Cardiochirurgia Valvulopatie Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Valvulopatia Mitralica Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Anatomy and Pathology 1. Crucial to understand the anatomy of the mitral valve in order or perform valve repair/surgery 2. Mitral valve is composed of five separate components: a. valvular leaflets b. annulus c. chordae tendinae d. papillary muscles e. left ventricular wall Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Pathology •Rheumatic Disease •Myxomatous Degeneration •Ischemic Valvulopaty •Endocarditis Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Rheumatic mitral stenosis Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Bacterial endocarditis on A2 Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE MS: Indications for Operation 1. asymptomatic patients are generally not recommended for operation 2. patients with severe mitral stenosis should undergo operation a. normal orifice is 4-6 cm2 b. 2-4 cm2 is mild c. 1-2cm2 is moderate d. < 1 cm2 is severe Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE MR: Indications for Operation •Acute symptomatic MR •Symptomatic or Asymptomatic Patients with LV Dysfunction: Type Mild Moderate Severe EF 0.5-0.6 0.3-0.5 <0.3 Systolic Dimension 40-50 mm 50-55 mm >55 mm (LV dysfunction will persist, symptoms diminish, risk increase) •Asymptomatic patients with atrial fibrillation or pulmonary hypertension (PAPm = >50 mmHg at rest, >60 mmHg exercise) Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Surgical Options •Valve replacement •Mortality 2-7% •Anticoagulation •Decrease LV EF •Valve Repair (always preferable – feasible in 70-90% of pts) •Mortality 2-3% •No anticoagulation •Preservation of LV EF Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE The Perfect Valve •Excellent hemodynamics •Non-thrombogenic •Durable •Unrestricted availability •Easily implantable •Silent function •Low cost Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Replacement Devices •Mechanical valves •Caged-ball •Monoleaflet •Bileaflet • Bioprostheses •Stented •Porcine •Pericardial Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE •Stentless •Porcine •Bovine Pericardial •Homograft •Autograft Kay Mitral Valve.Teflon mitral valve prosthesis with artificial chordae.Implanted 1959 Original Starr-Edwards Mitral Valve. Lucite cage. Silastic rubber ball occluder. Implanted 1960. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Braunwald Polyurethane mitral valve. First mitral valve replacement on March 11, 1960. Teflon chordae brought through the ventricular muscle and secured outside the heart Harken double cage ball valve. Implanted in 1960 St Jude heart valve. The most popular bileaflet mechanical valve. First implant 1977. Pyrolytic carbon leaflets and housing. Tungsten impregnated leaflets. Modifications: low profile sewing cuff, and rotatable housing St Jude Quattro tissue valve. Investigational stentless quadracuspid tissue valve for mitral valve replacement. Bovine pericardium. Carpentier-Edwards Perimount Mitral valve. Bovine pericardial tissue valve with Eligloy stent."Stress-free" fixation. Lower profile mitral tissue prosthesis. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Mitral Homograft Flow characteristics ball/cage < tilting dic < bileaflet Thrombogenic potential ball/cage > tilting disc > bileaflet Aortic < Mitral < both Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Anticoagulation Management (Machanical Prosthesis) •TIA is most common event •Standardization of coagulation management (INR) •Narrow therapeutic range: balance between thrombolic and bleeding risk •ACCP recommendations: INR 2.5-3.5 Aortic: 2.5-3.0 Mitral: 3.0-3.5 Both: 3.5-4.0 •Appropriate use of antiplatelet therapy Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Mechanism of mitral insufficiency (Carpentier Classification) Type I (normal leaflet motion) Type II (leaflet prolapse) Posterior leaflet Anterior leaflet Both leaflets Type III (restricted leaflet motion) Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE •Leaflet Prolapse (II): an excessive motion of a leaflet overriding the plane of the annulus in systole •Leaflet Restriction (III): an incomplete closure of a leaflet remaining beneath the plane of the annulus in systole Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Tecniche Riparative Mitraliche •Riparazioni Anatomiche •Annulus •Lembi •Corde Tendinee •Muscoli Papillari •Riparazioni Funzionali Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE The Quadrangular Resection Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Chordae Tendinae SHORTENING REPLACEMENT TRANSFER Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Galloway concludes, "The core concepts are: fix the leaflet pathology and remodel the annulus and you'll have a competent valve." Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Edge-To-Edge technique Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Valvulopatia Aortica Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Anatomy and Pathology 1. Crucial to understand the anatomy of the aortic valve in order or perform valve repair/surgery 2. Aortic valve is composed of five separate components: a. valvular cusps b. annulus c. Valsalva’s sinus d. sinus-tubular junction e. Aortic root Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Positions of the aortic valve leaflets at enddiastole and end-systole and of a single leaflet in profile during ejection as the leaflet moves from the closed position (0) to full opening. Note how the fully opened leaflet tends to produce a unifom diameter above the ventricular-arterial junction to reduce turbulence that otherwise would be increased by the sinuses of Valsalva. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Pathology •Congenital Malformation •Rheumatic Disease •Degeneration •Endocarditis Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Congenital Malformation Quadricuspid aortic(Ao)valve and unicuspid pulmonary (P)valve. The asterisk indicates the additional (fourth) leaflet of the aortic valve. Native aortic valve demonstrating fusion of the anterior commissure between the left and noncoronary cusps. A small thrombus is present on the right lunula of the left cusp. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Calcified Aortic Stenosis (Congenital Malformation) •Congenitally bicuspid or unicuspid, fused commissures, •heavy calcification, age 50-70 Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Rheumatic Aortic lesions •Fibrous thickening, •3-cusp valve, •mild calcification, •rheumatic fever history in 50% aortic steno-insufficiency Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Degeneration •Diffuse nodular calcification, •3-cusp valve, •no commissural fusion Macroscopic appearance of healed, fibrous commissural fusion between left coronary cusp (right, held by forceps) and noncoronary (left) cusp of aortic valve Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Endocarditis Infective endocarditis is defined as an infection of the endocardial surface of the heart, which may include one or more heart valves, the mural endocardium, or a septal defect. Endocarditis can be broken down into the following categories: •Native valve (acute and subacute) endocarditis •Prosthetic valve (early and late) endocarditis •Endocarditis related to intravenous drug use Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Parasternal short-axis view and its schematic drawing with color flow imaging from patient 1, showing perforation of the noncoronary cusp (N) of the aortic valve and aortic regurgitation (AR) after patch repair of an ostium primum atrial septal defect. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE AS: Indications for operation •Symptomatic Aortic Stenosis •CHF •Angina Pectoris •Syncope •Hemodinamic severity (ecocolorDoppler) •∆P ≥ 50 mmHg •Aortic Valve Area ≤ 0.75 cm2 or AVAi ≤ 0.4 cm2/m2 •Asymptomatic aortic stenosis – Hemodynamic severity with •Progressive LV enlargement •Decline of LV EF Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Aortic Incompetence · Cusp prolapse or cicatricial shortening of cusps with rolled edges · Annulo-aortic ectasia is a disease of the aorta rather than the valve itself · Dilation of sinus aorta, cystic medial necrosis, failure of coaptation of cusps Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE AI: Indications for Operation •Symptomatic Aortic Incompetence •Asymptomatic aortic regurgitation – Hemodynamic severity with •Progressive LV enlargement •Decline of LV EF •Hemodinamic severity (ecocolorDoppler) •LVEDD > 80 mm, LVESD > 55 mm, LVEF < 50% Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Aortic valve excision. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Mechanical prosthesis implantation. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE AORTIC HOMOGRAFT Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Homograft implantation: the “root” technique Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Pulmonary Autograft (Ross Procedure- 1967) Advantages Viable tissue, excellent hemodynamics Near 0% thromboembolism, growth potential Non-antigenic Pulmonary valve equal in strength as aortic valve Disadvantage Creating 2-way valve pathology from single valve disease Results Freedom from re-operation 81% at 8 years 5-10% annular dilatation and regurgitation Pulmonary homograft deterioration Technique Root replacement preferred Tailoring of aortic/pulmonary size mismatch Bolstering ring with Dacron strip Long-term follow-up still accruing Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE The Ross Operation Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Mechanical valved conduit implantation. A. The valve and proximal conduit are sutured to the annulus with everting, pledgeted mattress sutures. B. If necessary, the distal aortic layers are oversewn. C. A proximal coronary button is sutured to a hole made in the prosthesis. D. Completed graft with both coronary arterial buttons attached and the distal anastomosis finished. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Reimplantation of the aortic valve in patients with annuloaortic ectasia and aortic root aneurysm. (Reproduced with permission from David TE, Feindel CM, Bos J. Repair of the aortic valve in patients with aortic insufficiency and aortic root aneurysm. J Thorac Cardiovasc Surg 1995;109:345–52.) Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Cumulative distribution of prosthesis internal orifice size standardized to body surface area according to the Z-value. Normal native valve sizes are generally considered to be those constrained within the 95% confidence limits of normal values, corresponding to Z-values of –2 and +2. A, Overall distribution; B, distribution stratified by type of aortic valve prosthesis Thorac. Cardiovasc. Surg. 2000;119:963-974. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Aortic valve replacement: Is valve size important? B. Medalion Left ventricular mass index (LVMI) preoperatively (PREOP) and 8 months after (POSTOP) aortic valve replacement. The homograft and stentless valves expressed the maximum LVMI reduction. This is evident in all cases (A) and in patients with a preoperative LVMI of 180 g/m2 or less (B). In patients with a preoperative LVMI of 180 g/m2 or more (C) the homograft treatment achieved the best results. (I = intact; H = homografts; T = Toronto; F = freestyle; C = controls). “Left ventricular mass reduction after aortic valve replacement: homografts, stentless and stented valves” D. Maselli et al. Ann. Thorac. Surg. 1999;67:966-971. Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE Reparative aortic valve surgery. Reproduced from Duran and colleagues Cattedra di Cardiochirurgia UNIVERSITA’ DEGLI STUDI DI FIRENZE