Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
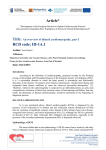
CARDIOMYOPATHIES COMPILED BY : DR .ALIREZA HOGHOOGHI CMP s: Heterogenous group of diseases of • myocardiom Associated with functional and structural • abnormalities Four main cmps DILATED CARDIOMYOPATHIES(DCM) • HYPERTROPHIC CARDIOMYOPATHIES(HCM) • RESTRICTIVE CARDIOMYOPATHIES(RCM) • ARRYTHMOGENIC RIGHT VENTRICULAR • DYSPLASIA Familial (genetic )and non familial (acquired)form of the diseases have been describe DCM Characterized by: enlargement of LV or LV OR RV Impaired systolic function of LV or LV and RV DCM can be famillial or acquired ¼ of DCM are familial(genetic mutation) Some specific mutations involve genes encode proteins of sarcomers,cytoskeeton ,nuclear membrane ,mitochondria and many remains unknown Mode of inheretance is typically A.D • NON FAMILIAL DCM HAS DIFFERENT CAUSES • Mostly believed to be a result of acute viral • myocarditis Exposure to cardiac toxins can also lead DCM Anthracyclines (doxorubicin).daunorbicin have dose dependant cardiac toxicity Long term exposure to alohol is an important • preventable cause of DCM • TABLE 59-7 -- CAUSES OF DILATED CARDIOMYOPATHY CARDIOVASCULAR DISORDERS • Systemic hypertension • Ischemic heart disease Valvular heart disease Myocarditis Peripartum cardiomyopathy TOXINS • Alcohol • Catecholamines Anthracyclines Radiation Cocaine ASSOCIATED SYSTEMIC DISEASES S • ystemic lupus erythematosus • Polyarteritis nodosa Rheumatoid arthritis Scleroderma Dermatomyositis MUSCULAR DISORDERS • Duchenne's muscular dystrophy • Becker-type muscular dystrophy Myotonic dystrophy Mitochondrial disorders HIGH-OUTPUT STATES Thiamine deficiency Thyrotoxicosis Severe anemia Arteriovenous fistulas/shunts Incessant tachycardia • • Deficiency of nutrients .thiamin vit C,selenium,phosphate,calcium Peripartum DCM is a form of idiopathic DCM • in last month of pregnancy or several month of delivery Pathogenesis is unknown autoimmune ,viral • myocarditis ,hemodynamic stress PROLONGED SVT OR VT CAN LEAD TO DCM • (tachycardia induced CMP) STRUCTURAL AND FUNCTIONAL CHANGES • REVERSE AFTER CONTROL OF HR Development of DCM can be gradual and many are asymptomatic first presentation is usually due to symptoms of heart failure :fatigue ,weakness,dyspnea,edema in some presenting episode is arrythmia On physical exam : Tachycardia is often present ,narrow pulse pressure ,tachypnea,jvp distention Laterally displaced apex,s3 gallop common ,murmur of MR and TR RALES ,PLEURAL EFFUSION , IN SOME RIGHT SIDED HF IS PROMINENT :ASCITES,HEPATOMEGALY ,EDMEMA ,ANASARA BNP LEVEL IS ELEVATED ECG NON SPECIFIC ST T CHANGE ECHO : EVALUATION OF LV SIZE AND • FUNCTION AND ABNORMALITY OF VALVES, AND LV THROMBUS SO DO MRI MYOCARDIAL BIOPSY IS INDICATED IF • ETIOLOGY OF DCM IS IN QUESTION IN PATIENT WITH STRONG FH REFERRAL FOR • GENETIC STUDY IS CONSIDERED THERAPY POTENTIAL REVERSIBLE CAUSES SHOULD BE • ADDRESSED LOOP DIURETICS FOR CONGESTED PERSONS • GOOD FOR SYMPTOMS BUT EFFECT OF • SURVIVAL HAS NOT BEEN EVALUATED ACEI.BETABLOCKERS ,HYDRALASINE NITRATES • ,ALDACTONE ,DIG ,CRT ,CRTD ,TRANSPLANT LV ASSISTED DEVICE HCM CHARACTERIZED BY LVH AND SMALL LV AND ABSENCE • OF AN APPARENT CAUSE FOR HYPERTROPHY COMON GENETIC DISEASE 1/500 AND IS A.D • >400 MUTATION IN 11 DIFFERENT GENE • MUTATION OF BETA MYOSIN HEAVY CHAIN IS • FREQUENT THERE IS SPORADIC FORM • MICROSPIC PHENOTYPE .CARDIOMYOCYTE • HYPERTROPHY ,MYOFIBRILLAR AND INTERESTITIAL FIBROSIS NEW ADDED TO HCM METABOLIC STORAGE DISEASE THAT RESULT • IN CHANGES IN MYOCARDIAL APPEARANCE WHICH RESEMBLES HCM GYCOGEN STORAGE STORAGE DISEASE • LYSOSOMAL STORAGE DISEASE • DISORDER OF FATTY ACID METABOLISM PHENoTYPICAL EXPRESSION Is DIFFERENT BECAUSE OF DIFFERENT PENETARTION Main pathophysiologic abnormalities seen in • HCM are LVOT OBSTRUCTION DIASTOLIC DYSFUNCTION .MR .ARRYTHMIA • Presentation Some are asymptomatic • Symtom result of lvoto and diastolic dysfunction • Most frequent dyspnea on exertion,which causes • marked lv filling pressure and pulmonary venous pressures and congestion Ischemic chest pain in absence of CAD • Syncope and presyncope • In some sudden death due to arrythmia is first • presentation Physical exam Bisferiens pulse • Forceful and sustained apical impulse • Decreased complince of the LV during atrial • contraction may lead to an audible s4 Harsh crescendo and decrscendo sm best • heard in lsb radiation to base of the heart May be apical holosystolic murmur of MR • Intensity of murmur will increase with valsalva ,standing and use of tng or inotrops Intensity of murmur will decrease with squating ,volume loading ,use of beta blockers Ecg in hcm :increased QRS voltage suggestive of LVH .SECONDARY ST CHANGE AND T INVERSION .,PSUDOINFARCT PATTERN WITH Q IN INF ,LAT OR ANT LEADS ECHO AND MRI ARE HELPFL IN CONFIRMING THE • DIAGNOSIS ECHO IS USEFUL IN SCREENING • CATH IF ECHO IS NOT ADEQUATE AND CAN CONFIRM • INTRA CAVITARY GRADIENT MANAGEMENT IS AIMED TO REDUCING TH • LVOTOBSTRUCTION ,IMPROVING DIASTOLIC DYSFUNCTION AND REDUCING RISK OF SUDDEN DEATH BETABLOCKERS AND CALCIUM CHANNEL • BLOCKERS AND DISOPYRAMIDE CAN REDUCE SYMPTOMS PPM, SURGERY SEPTAL MYECTOMY,ALCOHOL ABLATION ICD FOR SUDEN DEATH : • 1.PRIOR CARDIAC ARREST • 2.SUSTAIN VT • 3.>30 MM VENTRICULAR THICK NESS • 4.SYNCOPE • 5.FIRST DEGREE RELATIVE SUDDEN DEATH • RCM RCM IS RARE • CHARACTERIZED BY IMPAIRED VENTRICULAR • FILLING OR DECREASED DIASTOLIC VOLUME OF EITHER OR BOTH VENTRICLE VENTRICULAR PRESSURE RISE SIGNIFICNT • SYSTOLIC FUNCTION USUALLY IS PRESERVED • ARE FAMILLIAL OR NONFAMILLIAL • ONE OF THE COMMON FORM OF FAMILLIAL FORM IS FAMILIAL AMYLOIDOSIS<TRANSTHYRETIN AND APOLIPOPROTEINS FAMILIAL HEMOCHROMATOSIS • MUTATION IN DESMIN • AQUIRED • FORMS:AMYLOIDOSIS,SARCOIDOSIS,CARCINOI D HEART DISEASE ,SCLERODERMA ENDOCARDIAL PATHOPHYSIOLOGY OF • STIFFNESS IS ALSO PRESENT:HYPEREOSINOPHILIC SYNDROME DIAGNOSIS OF RCM SHOULD BE CONSIDERED IN PATIENT WITH PREDOMINANTLY RV FAILURE WITHOT EVIDENCE OF CARDIOMEGALY OR SYSTOLIC DYSFUNCTION CONSTRICTIVE PERICARDITIS CAN PRESENT • SIMILARLY TO RCM TREATMENT IS FOCUSED ON ALLEVIATATING • THE SYMPTOMS OF HEART FAILURE ARVD IS A.D • MALE PREDOMINANCE • PROGRRESIVE REPLACEMENT OF RV MYOCARDIUM BY • FIBROUS AND ADIPOSE TISSUE INSOME INVOLVES LV IN THESE PATIENT PRESENTATION MAY RESEMBLE DCM PREVALNCE 1/1000 TO 1/5000 • PRESENTING IN YOUNG ADULT • PRESENTING SYMPTOMS IS USUALLY ARRYTHMIA • ,PALPITATION ,SYNCOPE,,SUDDEN DEATH ,SYMPTOM OF RV FAILURE IS RARE DIAGNOSIS IS MADE ,BY CLINICAL PRESENTATION Resting ECG • FAMILY HISTORY • IMAGING STUDY • ECG USUALY NORMAL BUT SOME MAY HAVE • INCOMPLETE OR COMPLETE RBB AND EPSILON WAVE AND INVERTED T WAVES IN PRECORDIAL VT MOOMORPHIC WITH LBBB PATTERN • TREATMENT BY ICD • CARDIOMYOPATHIES •





















































![[INSERT_DATE] RE: Genetic Testing for Dilated Cardiomyopathy](http://s1.studyres.com/store/data/001660325_1-0111d454c52a7ec2541470ed7b0f5329-150x150.png)


![[INSERT_DATE] RE: Genetic Testing for Dilated Cardiomyopathy](http://s1.studyres.com/store/data/001478449_1-ee1755c10bed32eb7b1fe463e36ed5ad-150x150.png)