Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Anesthesia
In Children With
Congenital Heart Disease For
Non-cardiac Surgery
Dr. Fady Adib
Lecturer Of Anesthesia
Ain-Shams University
Oct. 2012
The question facing anesthetists
are:
1 . Should the patient be referred to
specialist cardiologist before surgery?
2 . Should surgery be performed in a center
specializing in congenital cardiology?
3 . How should anesthesia be conducted
safely in the presence of congenital heart
disease?
INTRODUCTION
The Incidence of CHD is about 1%
of the newborn infants
- Surgery:
- Noncardiac conditions ( inguinal hernia,
circumcision, or tonsillectomy).
- Associated noncardiac congenital
anomalies (orthopedic or genitourinary).
- Due to advances in diagnosis, medical, critical
and surgical care for CHD
- Therefore, it is common for patients with CHD
to present for non-cardiac surgery, and even in
patient with corrected CHD significant residual
problems (arrhythmias, ventricular dysfunction,
shunts, valvular stenosis, and PH) may be exist.
Anatomical & Physiological
Differences
CVS: Anatomical Differences
- Myocardium is less compliant:
Cardiac Output is H.R. dependent.
- It can’t withstand a volume load.
- Decreased sympathetic innervation:
catecholamine stores
Autonomic Development
- Beta receptors develop with age
- alpha receptors less developed
So V.C response to volume loss is decreased
- Parasympathetic response supervens
- Net result:
- Volume load
heart failure
- Volume loss
decrease
vasoconstriction
- Hypotension
CLASSIFICATION OF CHD
I- Acyanotic congenital heart disease:
1- ASD
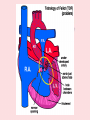
2- VSD
3- PDA
II- Cyanotic congenital heart disease:
1- Tetralogy of Fallot, with severe right
ventricular outflow obstruction
2- TGA
3- Pulmonary atresia or severe stenosis
4- Tricuspid atresia with pulmonary stenosis
5- Truncus Arteriosus
Pathophysiological classification
of congenital heart disease
- Shunt lesions
- Mixing lesions
- Obstructive lesions
- Regurgitation lesions
Shunt lesions
Intracadriac
Extracardiac:
e.g. ASD, VSD
e.g. PDA
- Direction & magnitude:
depends on
size of shunt orifice
pressure on both sides of the shunt
- Lt.-to-Rt. Shunt ( e.g. VSD,PDA)
- Rt.-to-Lt. Shunt (e.g. Fallot 4)
OVERLOAD
VOLUME OVERLOAD
PRESSURE
..Shunt lesions.. (continued)
Lt-to-Rt shunt
e.g. ASD, VSD
- Volume overload on
pulmonary circulation
- Increased cardiac
work of Rt. Ventricle
- Excessive pulmonary
blood flow=++ PVR
Rt-to-Lt shunt
e.g. F4
- ↓ Pulmonary blood
flow=
hypoxemia
- Pressure overload of
the Rt. ventricle
Mixing lesions
(large orifice)
- e.g. TGA, Univentricular heart
- Direction & Magnitude:
Depend on PRESSURE on both sides of the
lesion
- Usually CYANOTIC
- With VOLUME & PRESSURE overload
Obstructive lesions
- e.g. Aortic stenosis, Coarctation of Aorta
- Pressure overload
ventricular hypertrophy
impaired coronary perfusion
systemic hypotension
Regurgitation lesions
(uncommon)
- Volume overload
dilatation
ventricular
Once full details of the anatomy, surgical history and
current pathophysiology are obtained patient can be
divided into the following categories:
1 . Congenital heart disease, yet to be surgically
treated.
2 . Surgically corrected, symptom free with no new
development.
3 . Surgically corrected, symptomatic heart diseases
4 . Surgically palliated. Symptoms stable with no new
development
5 . Surgically palliated with severe symptoms or no new
development
Types of Cardiac Surgery
Biventricular
Univentricular
Usually Palliative
e.g. Shunts, Banding
•Problems encountered:
Usually complete repair
( Corrective )
Debubbling & Antibiotic coverage,
As the lesion is still persistent e.g. VSD
- Corrective surgery: Correct
anatomy
- Palliative surgery: The aim is to
increase or decrease pulmonary blood
flow
Corrective Surgery
Corrected ASD VSD PDA: Near normal
patient. Only needs antibiotic prophylaxis.
Repaired TOF: Residual defects: VSD,
outflow tract obstruction, pulmonary regurge,
,Heart block
Corrected coarcitation usually require long
.term treatment of hypertension
Palliative surgery
Decrease PBF: Pulmonary artery
banding (VSD)
Increase PBF: In Pulmonary atresia
BT shunt: Subclavian artery to
.Pulmonary artery
Gllen: SVC to Pulmonary artery
Fontan after Gllen IVC to Pulmonary
artery
Physiology of different types
of circulation
- Normal or ‘series’ circulation.
-
- Parallel or ‘balanced’ circulation.
- Single-ventricle circulation
-
-
Risk classification
increased risk of mortality and morbidity.
- factors associated with a high risk of
perioperative complications,
- {disease complexity, }
Most Important
- {physiological status,}
- type of surgery, young age, and Hospital Stay .
Complexity of heart disease
- single-ventricle physiology
- balanced circulation physiology
- cardiomyopathy
- aortic stenosis
Physiological status
Physiological status can be divided into four
major risk factors:
- Cardiac failure
- Pulmonary hypertension
- Arrhythmias
- Cyanosis
ANESTHETIC MANAGEMENT
- Perioperative management requires a team
approach
- CHD is polymorphic and may clinically
manifest across a broad clinical spectrum
- The plane of Anesthetic Management includes
the following:
A - Preoperative Management
B - Intraoperative Management
C - Postoperative Management
Preoperative Anesthetic Considerations
1- Complete history and physical examin.
2- Review all investigations
3- Hydration should be maintained
4- All cardiac medication except possibly digitalis ,ACE
and diuretics should be continued until surgery
5- Premedication should be give particularly to patients
at risk for right to left shunt
6- Antibiotic prophylaxis against endocarditis must be
given
Preoperative Anesthetic Management:
A- History
B- physical examination
C- Investigations
D- Premedications
E- Fasting Guidelines
HISTORY & PHYSICAL EXAMINATION
- Assess functional status
- daily activities
- exercise tolerance
- ↓ cardiac reserve
- cyanosis
- respiratory distress during feeding
- Cyanosis
- Dyspnea
- Fainting attack
- Fatigue
- Palpitations
- chest pain
- Syncope
- Abdominal fullness
- Leg swelling
- Medications
- Vital signs
- Airway abnormality
- Associated extracardiac
congenital anomalies
- Tachypnea, dyspnea, cyanosis
- Squatting
- Clubbing of digits
- Heart murmur (s)
- CHF:
- Jugular venous distention.
- Hepatomegally
- Ascitis
- Peripheral edema
MRI
Laboratory
Evaluation
12 Lead ECG
INVESTIGATIONS
chest X – Ray
Echocardiography
Cardiac Catheterization
Regarding investigations of CHD patients for non-cardiac surgery:
A- Chest X – Ray has no rule
B- Cardiac Catheterization is the first choice for diagnosis of
CHD
C- Echocardiography non invasive method for diagnosis of CHD
D- MRI cannot give us idea about pulmonary veins
IM Premedication for CHD patients presenting for non-cardiac
suergery:
A- Cooperative or unable to take orally
B- Ketamine 1mg/kg
C- Midazolam 5 mg/kg
D -Glycopyrrolate or Atropine 0.02 mg/kg
Procedural antibiotic prophylaxis is required in patients with
A- Aortic valve replacement
B- Mitral valve prolapse with regurge
C- Previous history of infective endocarditis
D- Ostium secundum ASD
AHA guidelines for bacterial endocarditis Prophylaxis in
patients with cardiac conditions
Endocarditis prophylaxis recommended
Endocarditis prophylaxis not recommended
High-risk category
- Complex cyanotic congenital heart disease :
Transposition of the great vessels
Tetralogy of Fallot
- Surgically created systemic-to-pulmonary
shuntsor conduits
- Prosthetic, Bioprosthetic, Homograft valves
- Previous bacterial endocarditis
Negligible-risk category
- Physiologic, or functional heart murmurs
Moderate-risk category
- Other congenital cardiac anomalies
- Acquired valvular dysfunction
- Hypertrophic cardiomyopathies
- Mitral valve prolapse with valvar- Regurg
- Surgical repair without residua beyond
6 months : ASD, PDA,VSD
- Cardiac pacemaker or
- implanted defibrillator
- Isolated secundum atrial septal defect
- Mitral valve prolapse without reg.
- Previous coronary artery bypass surgery
- Previous rheumatic heart disease
without valvular dysfunction
AHA guidelines for antibiotic prophylaxis: dental, oral,
Respiratory tract and esophageal procedures
Standard prophylaxis
Amoxicillin 1 h before procedure
-Children: 50 mg/kg p.o.
-.Adults: 2.0 g p.o
Unable to take oral
medications
Ampicillin within 30 min before
procedure
- Children: 50 mg/ kg i.m. or i.v.
-.Adults: 2.0 g i.m. or i.v
Allergic to penicillin
Clindamycin 1 h before procedure
Children: 20 mg/kg p.o.
Adults: 600 mg p.o.
OR Azithromycin or clarithromycin 1 h
before procedure
-Children: 15 mg/kg p.o.
- .Adults: 500 mg p.o
Unable to take oral
medications
AND allergic to penicillin
Clindamycin within 30 min before
procedur
-Children: 20 mg/ kg i.v
- .-Adult: 600 mg i.v.
AHA guidelines for antibiotic prophylaxis: genitourinary
and gastrointestinal procedures
High risk patients
- within 30 min before procedure
- Children: Ampicillin 50 mg/ kg .and gentaicin 1.5
mg/kg i.m or i.v
- Adults: Ampicillin 2.0 g and gentamicin 1.5
mg/kg i.m or i.v
High risk patients Allergic
to penicillin
- Complete infusion 30 min before procedure
- Children: Vancomycin 20 mg/kg i.v over 1-2 hr
gentamicin 1.5 mg/kg i.m or i.v
-Adults: Vancomycin 1g/kg i.v over 1-2 hr
gentamicin 1.5 mg/kg i.m or i.v
Moderate risk patients
- Ampicillin within 30 min before procedure
- Children: 50 mg/ kg i.m. or .iv
- Adults: 2.0 g i.m or i.v
Moderate risk patients
AND allergic to penicillin
- Complete infusion 30 min before procedure
- Children: Vancomycin 20 mg/kg i.v over 1-2 hr
-Adults: Vancomycin 1g/kg i.v over 1-2 hr
Anesthetic Management
A - Preoperative Management
B - Intraoperative Management :
1- Monitoring
2- Choice of anesthetic agent
3- Maintenance of anesthesia
4- Emergence from anesthesia
Anesthetic Management
Preoperative Assessment
- Associated congenital anomalies (difficult
airway)
- Chest: signs of H.F.& chest infection…postpone
- Liver:
●enlarged in Rt. Sided failure
●shrunken in Lt. sided failure, diuretics,
↓feeding
- Cyanotic spells
- Acute hypertensive pulmonary crisis
Anesthetic Management
Investigations
- Hematocrit:….thromboembolism
- Electrolytes:…..arrhythmias..(should be
corrected)
- Blood gases:…cyanotic may be acidotic
- Echocardiography: satisfactory in simple cases
- Catheterization:
- Coagulation profile: cyanotic patients usually
suffer from coagulopathies.
Premedication
-
-
-
Oral Premedication:
- Midazolam 0.25 -1.0 mg/kg
- Ketamine 2 - 4 mg/kg
- Atropine 0.02 mg/kg
IV Premedication:
- Midazolam 0.02 - 0.05 mg/kg titrated in small increments
- Ketamine 1-2 mg/kg
IM Premedication:
- Uncooperative or unable to take orally
- Ketamine 5 – 10 mg/kg
- Midazolam 0.2 mg/kg
- Glycopyrrolate or Atropine 0.02 mg/kg
Fasting Guidelines
Anesthetic Management
Premedication
- Fasting: clear sugar fluid allowed till 4
hours
- ↓ 6 months: No premedication
- 6-9 months: optional e.g. to avoid spell
or crisis
- ↑9 months:
-atraumatic (oral midazolam)
-IM: ketamine 2mg/kg
add Atropine 0.02mg/kg
Anesthetic Management
O.R. preparation
- Temperature control: mattress & O.R. temp.
- Anesthetic machine: with O2, Air, N2O
- Infusion set…… free of air bubbles
- Drugs: Atropine, Bicarb., Epinephrine,
Phenylephrine
- Inotropic infusion should be premixed before
induction in high risk patient (e.g.Dobutamine)
Anesthetic Management
Monitoring & Lines
- ECG
- Pulse Oximetry: inaccurate in deep
hypothermia
- Invasive B.P.: Lt. Radial, Rt. Radial,
Femoral art.
- CV. Cannulation: Rt. & Lt. IJV, Femoral vein
- Temperature: central & peripheral
- Urine output:
- Capnography:
- Blood gases & electrolytes.
Monitoring
Non-invasive
- Clinical observation
- ECG
- NIBP
- Pulse oximetry
- Precordial stethoscope
- Continuous airway
manometry
- Multiple site
temperature
measurement
Invasive
- Volumetric urine
collection
- Art. catheterization
- CVP
- PAC
- TEE
Inraoperative management
The goals of Intraoperative
management
- Prophylaxis against Subacute bacterial
endocarditis.
- Prophylaxis against Air bubble embolism.
- Hemodynamic management.
PVR
SVR
Contractility
Air bubble precautions
- Check and remove all air bubbles from IV
tubing, injection ports, and stopcocks
- Connect the IV tubing to the venous
cannula while there is a free flowing IV
fluid and blood.
- Before IV injection into the cannula, small
amount if fluid is injected into the hub of
the cannula.
Air bubble precautions
Aspiration before injection to clear any air.
Hold the syringe upright to keep the bubbles
away.
Do not inject the last milliliters from the
syringe.
Do not leave the central line open to air.
N2O is better avoided.
Hemodynamic
management
Left to right shunts:
( pulmonary blood flow)
- The aim is to prevent:
in SVR
in PVR
contractility
Avoid
vasodilators
high FiO2
hypocapnea
and alkalosis
Right to left shunts:
( pulmonary blood flow)
-
The aim is to prevent:
in SVR
in PVR
contractility
Avoid
Sympathetic
stimulation
low FiO2
hypercapnea
.acidosis
Avoid N2O
Anesthetic Management
Induction
- Aim: to preserve SVR & PVR
- Method:
● Inhalational: Sevoflurane
● I.V.: ketamine 2 mg/kg + fentanyl 2-3μg/kg+
Pancuronium 0.1 mg/kg
- Antibiotic Prophylaxis:
- Intubation: Oral/ Nasal (postoperative)
- Corticosteroids: decrease systemic inflammatory
response
The effect of shunt on the speed of
induction of anesthesia:
- In patients with a right-to-left shunt:
Inhalation induction is prolonged .
Intravenous induction is more rapid.
- In patients with left-to-right shunting, the
speed of inhalation or intravenous induction
is not changed .
Factors Affecting PVR
Factors
Increasing:
- PEEP
- High airway
pressure
Atelectasis,hypoxia
,hypercarbia
- Acidosis
- Catecholamine
-High hematocrite
Factors
Decreasing:
- No PEEP
- Low airway
pressure
- High FiO2,
hypocarbia
- Alkalosis
- Vasodilators
- Low hematocrite
- Nitric oxide
Anesthetic Management
Maintenance
- Patient with Poor Myocardium:
- Narcotic based....Extubation not advisable
- Patient with Good Myocardium:
- Inhalational (isoflurane, sevoflurane)
- Most Stressful Situations:
- Skin incision
- Sternotomy
- Major vessels cannulation (Aorta,
SVC,IVC)
Choice of anesthetic Regimen
Development of anesthetic regimen
is based on various factors such as
presence and direction of shunts ,
arrhythmia , pulmonary HF,
circulation,
and lowering or
maintenance of PVR
●
Choice of Anesthetic Agent
Intravenous
anesthetics
•
Volatile
anesthetics
Muscle
relaxants
Ketamine : No change in PVR in children when airway maintained & ventilation supported
Sympathomimetic effects help maintain HR, SVR, MAP and contractility
Greater hemodynamic stability in hypovolemic patients
Copious secretions (laryngospasm)
•
Etomidate : Induction dose of 0.3mg/kg no change in mean pulmonary artery pressure and
PVR, pulmonary blood flow, PHT or myocardial function
•
Propofol : decrease in SBP and SVR, and increase in SBF in all patients, whereas HR ,PAP, PBF
remained unchanged
•
OPIOD: Excellent induction agents in very sick children No cardiodepressant effects if
bradycardia avoided Fentanyl 15-25 µg/kg IV , Sufentanil 5-20 µg/kg IV
•
Barbiturates : Not recommended in patients with severe cardiac reserve
Choice of Anesthetic Agent
(Cont.)
- Desflurane Pungent , PAP and PVR, Less myocardial depression than Halothane HR , SVR
- Halothane PBF not affecting PVR, Depresses myocardial function, alters sinus node function,
sensitizes myocardium to catecholamines
- Isoflurane Pungent, PAP not affecting PVR, Less myocardial depression than Vasodilatation
leads to SVR → MAP , HR which can lead to CI
- Sevoflurane Less myocardial depression than Halothane, more in PAP compared
with
isoflurane, No HR, Mild SVR, Can produce diastolic dysfunction
- Nitrous oxide At 50% concentration does not affect PVR and PAP in children
Avoid in children with limited pulmonary blood flow, PHT or myocardial function
Neuromuscular Blocking Drugs
Depolarizing
- Succinylcholine in pediatric
controversial is
- If used should be with atropine,
to avoid associated bradycardia or sinus arrest
- also if used with potent narcotic
atropine should be used
avoid severe to
bradycardia in children with
CR
Nondepolarizing
- Atracuruim and vecronium: have few
cardiovascular side effects in children
when given in recommended doses.
- Pancuronuim if given slowly doesn't
produce HR or BP changes. if given as
bolus doses it can produce tachycardia ,
↑BP (through sympathomimetic effect )
-Cisatracuruim and Rocuroinuim: safe
Anestheia of Fallot patient:
- The aim is to prevent intraoperative cyanotic
spells.
- Avoid prolonged fasting
- Heavy sedative premedication.
- Intravenous induction.
- Ketamine, Fentanyl, Pancronium, Halothane.
- Adequate intravascular volume.
- Avoid systemic vasodilatation.
- Adequate anesthetic depth to avoid
sympathetic stimulation.
Management of intra operative
cyanotic spells in Fallot patient
- Direct abdominal or aortic compression
- IV vasoconstricror as ephedrine,
phenylephrine, or dopamine
- IV fluid.
- Deep level of anesthesia.
- Beta adrenergic blockers as osmolol or
propranolol
REGIONAL ANESTHESIA &ANALGESIA
• Considerations :
- Coarctation of aorta considerations
- Childern with chronic cyanosis risk of
coagulation abnormality
- VD : which can:
1- be hazardous in patients with significant
AS or left-sided obstructive lesions
2- Cause oxyhemoglobin saturation in R-L
shunts
Postoperative Anesthetic Management
- Supplemental O2 and maintain patent airway.
- In patients with single ventricle titrate SaO2 to 85%.
Higher oxygen sat. can PVR PBF SBF
Pain catech. which can affect VR and shunt
direction
Pain infundibular spasm in TOF RVOT
obstruction cyanosis, hypoxia, syncope, seizures,
acidosis and death
Anticipate conduction disturbances in septal defects
Remember
Management of
- Acute hypertensive pulmonary crisis:
- Ventilatory manipulation: reduce PVR
(PaO2, PaCO2, PH, Lung volumes)
- Drugs: Milrinone, Isopril, PgE2
Remember
Management of
- Intraoperative Cyanotic Spells
-Increase S.V.R.: by direct aortic compression ±
vasopressor
(phenylephrine, ephedrine…..)
-Reduce infundibular obstruction by ß-Blockers
(esmolol, propranolol…),
OR Halothane
-Deepen the level of anesthesia.
-Adequate hydration (ample fluid and decrease viscosity)
SUMMARY
- Familiarity with the CHD pathophysiology,
adequate preoperative preparation, choice of
monitors, induction, maintenance , emergence
from anesthesia, and plans for the postoperative
period to avoid major problems in anesthetic
management
- A wide variety of anesthetic regimens is used for
patients with congenital heart disease (CHD)
undergoing cardiac or non-cardiac surgery, or
other diagnostic or therapeutic procedures. The
goal of all of these regimens is to produce
anesthesia or adequate sedation, while
preserving systemic cardiac output and oxygen
delivery