Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Kidney stone disease wikipedia , lookup
Kidney transplantation wikipedia , lookup
Interstitial cystitis wikipedia , lookup
Chronic kidney disease wikipedia , lookup
IgA nephropathy wikipedia , lookup
Renal angina wikipedia , lookup
Urinary tract infection wikipedia , lookup
Autosomal dominant polycystic kidney disease wikipedia , lookup
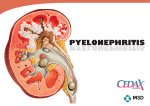
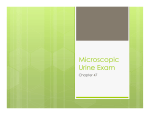
Approach to the Children with Urinary Tract Infection By Seyed Taher Esfahani,MD Professor of Pediatrics Tehran University Of Medical Sciences Definition of UTI UTI is defined by the presence of bacteria in bladder urine DEFINITION OF URINARY TRACT INFECTION The reference standard for urinary tract infection (UTI) is the isolation of a pure growth of bacteria in an uncontaminated sample of urine using semiquantitative culture methods The Importance of Pediatric UTIS UTIS are common in children UTIS may have nonspecific sign and symptoms UTIS have tendency to recur UTIS can lead to renal damage Prevalence • UTIs are relatively common in infants and young children. • The risk before puberty is 3–5% in girls and 1–2% in boys . • In young febrile infants aged less than 24 months the prevalence is 3–5%. • Prevalence is different depending on age and gender. Pathogenesis of UTI UTI is most often an ascending process except: During first 8-12 weeks of life Immunocompromised children Bacteriemia from an extra urinary site: skin ,heart , gastrointestinal, skeleton E.Coli E.Coli BLADDER CONTMINATION BLADDER INFECTION ( Vesicoureteral reflux ) ( Vesicoureteral reflux ) PELVICALYCEAL CONTAMINATION ( Intrarenal reflux) RENALMEDULIARY CONTAMINATION RENALINFECTION REFLUX NERPHROPATHY Bacterial inoculation of renal parenchyma Complement activation Immune response Chemo taxis - opsonization Phagocytosis…….........……. Intravascular Granulocyte aggregation Super oxide release Lysozyme Release Bacterial killing Tubular cell death Focal Interstitial invasion RENAL SCAR ischemia Classification of UTI 1- symptomatic: acute pyelonephritis acute cystitis unspecified UTI 2- Asymptomatic bacteriuria Approach to the children with UTI 1-Diagnosis of UTI 2-Determination of the site of infection 3-Search for the cause of UTI 4-Treatment •False positive diagnosis of UTI may lead to unnecessary treatment ,invasive and expensive clinical and radiological examinations •False negative diagnosis of UTI increases risk of scarring, hypertension, complications of pregnancy and end stage renal disease Methods to Obtain Urine Specimens • The gold standard for obtaining urine in an infant is by suprapubic aspiration. Complications are rare with the use of ultrasound guidance. • Urinary catheterization is also a very reliable method for obtaining urine without contamination, • Clean-catch mid-stream urine specimens can be collected in toilet-trained children. • The collection of urine in ‘‘collection bags’’ adhesively attached to the the perineal area The American Academy of Pediatrics The collection of urine in‘‘collection bags’’ adhesively attached to the the perineal area has no role in the diagnosis of childhood UTIs. The high contamination rate, with ‘‘false positive’’ rates as high as 86% may lead to unnecessary hospitalizations, and/or inappropriate clinical and radiological testing. the American Academy of Pediatrics Suprapubic aspiration Suprapubic aspiration Bacteria that Cause UTI in Children • E.Coli 60-80% • The other common bacteria are: Proteus, Klebsiella, Staphylococcus saprophyticus, Enterococcus, and Enterobacter Urinalysis for Immediate Diagnostic Information Dipstick testing: nitrite, leucocytes protein and blood Microscopic examination: WBC, RBC, Bacteria, Cast Localization of the UTI(1) • The differentiation between upper(pyelonephritis) and lower (cystitis) UTI is very important. • It particularly has major clinical implications in young children. The risk of renal scarring is significant with pyelonephritis, and not a concern with cystitis. Localization of the UTI(2) Clinical signs Pyelonephritis: high fever, chills, back or flank pain, renal tenderness, varied gastrointestinal symptoms: diarrhea, vomiting, and nausea, In addition, neurological symptoms such as irritability, and seizures (particularly with high fever) may exist. Localization of the UTI(3) Clinical signs Bacterial cystitis: There is rarely fever >38 Common findings include low grade abdominal pain and bladder/voiding symptoms such as frequency, pain with micturation, suprapublic discomfort, difficulty in voiding (retention) or hesitancy, urgency, and enuresis. Specific Clinical Signs of UTIs in Neonates and Infants The symptoms are nonspecific and require a high degree of clinical suspicion. They include fever, poor feeding, failure to thrive, abdominal pain, haematuria, and malodorous urine. Jaundice may be an early diagnostic sign of UTI in infancy • unexplained fever Localization of the UTI(4) Biological Tests • decreased renal concentrating capacity in pyelonephritis • Specific antibodies to the infecting bacteria • An elevated erythrocyte sedimentation rate, a positive Creactive protein, • An elevated peripheral WBC count with an increased absolute neutrophil counts • Recently a high procalcitonin concentration was described as a validated predictor of acute pyelonephritis Serum procalcitonin • Procalcitonin is an acute inflammatory marker with a sensitivity of 70-95% and a specificity that approaches 90% for renal involvement compared with results of DMSA scan in infants and children with febrile UTI. Although less sensitive than CRP, procalcitonin is more specific for the diagnosis of acute pyelonephritis. Procalcitonin values are better correlated with long-term renal scarring than CRP. Serum procalcitonin • Procalcitonin levels near 0.5 ng/mL may not consistently correlate with acute pyelonephritis. As procalcitonin levels increase, the severity of renal lesions on DMSA increases. • Higher levels of procalcitonin predict VUR in infants and children at the onset of pyelonephritis Serum and urinary interleukin (IL)-6 and IL8 Serum and urinary interleukin (IL)-6 and IL-8 are correlated with renal involvement in infants and children with UTI with high sensitivity (81-88%) and acceptable specificity (7883%). These markers are not reliable in neonates with suspected acute pyelonephritis. Imaging Tests in Localizing the Site of Infection 1-Renal cortical scintigraphy 2-Renal ultrasound 3- Computed Tomography 4-Magnetic resonance Imaging Imaging of pyelonephritis RUS and IVU are relatively insensitive for detection of pyelonephritis Radionuclide cortical scan, Computed tomography, magnetic resonance imaging are more sensitive Application of • 99mT -DMSA c 99mT -DMSA c is the gold standard for the identification of pyelonephritis and renal scars • Determining split renal function • To identify and character renal infarcts horseshoe kidney pelvic kidney crossed fused ectopia National institute of Health and Clinical Excellence (NICE): Clinical Guideline, August 2007 The use of DMSA scintigraphy scanning is only recommended by the NICE clinical guidelines in situations when it is clinically important to confirm or exclude acute pyelonephritis, and when the power Doppler ultrasound is not available or the diagnosis still cannot be performed guidance.nice.org National institute of Health and Clinical Excellence (NICE): Clinical Guideline, August 2007 Despite a large body of published literature, the role of radionuclide renal scans in the clinical management of the child with UTI still is unclear. Most of the time such imaging has no role in the specific management of childhood UTIs. guidance.nice.org Factors that may complicate interpretation of 99mTc-DMSA • Fetal lobulation • The splenic impression • The relatively decreased uptake of the poles of normal kidney Causes of defects in DMSA • • • • • • • • Acute pyelonephritis Renal scars Cysts Hydronephrosis Infarcts Masses Dysplastic half of a duplex kidney Proximal tubulopathies DMSA • Planar scintigraphy • Single photon emission computed tomography (SPECT) SPECT Cortical Scintigraphy • Superior sensitivity for detecting renal scars • Higher rates of false positive results • The increased imaging time with SPECT may necessitate sedation Split renal function in DMSA scintigraphy Normal split function = 50% ± 6% Renal Ultrasound Most of the time, conventional renal ultrasound is insensitive for the diagnosis of pyelonephritis. Signs of pyelonephritis include focal or diffuse renal enlargement, an abnormal cortical echogenicity mostly areas of increased echogenicity which may mimic a renal mass Renal Ultrasound •Power Doppler ultrasound is more sensitive than gray scale ultrasound: “Pyelonephritis is associated with renal ischemia. It is seen as a hypovascular zone in renal cortex”. Normal Kidney Gray-scale ultrasound shows diffuse enlargement of the left kidney, which measures 10.3 cm, and a loss of corticomedullary differentiation Pyelonephritis. Transverse gray-scale sonography of the right kidney demonstrate two wedge-shape areas of decreased echogenicity (arrow) Renal abscess Renal abscess Longitudinal gray-scale ultrasound of the right kidney reveal presence of a well-defined hypoechoic lesion Renal abscess. transverse (B) gray-scale ultrasound of the right kidney reveal presence of a well-defined hypoechoic lesion (A) near the superior pole Fungal Ball Power Doppler interrogation shows decreased perfusion to the lower pole of the left kidney Pyelonephritis. Transverse gray-scale (A) and color flow Doppler (B) sonography of the right kidney demonstrate absence of color flow, consistent with multifocal pyelonephritis. Renal abscess power Doppler image (C) demonstrates an increased peripheral vascularity Power Doppler ultrasound. Triangular area of cortical ischemia which is well correlated with the results of DMSA Scintigraphy Computed Tomography The features of pyelonephritis by CT have been well described: After intravenous contrast, areas of infected renal parenchyma have decreased contrast enhancement due to the renal ischemia, whereas normal renal parenchyma becomes brighter CT:Right kidney is markedly enlarged and has a wedge-shaped area of low attenuation Enhanced CT at the level of the kidneys demonstrates an area in the posteromedial aspect of the right kidney with diminished enhancement(arrow), consistent with the clinical suspicion of pyelonephritis. Magnetic resonance imaging After IV gadolinium contrast the lesions of pyelonephritis remain bright and the normal renal parenchyma is dark. MRI / Acute pyelonephritis Note clumps of small focal lesions irregularly distributed about kidney. Some elevated. .Acute pyelonephritis Acute Pyelonephritis Acute Pyelonephritis Diagrammatic representation of features of renal scars seen in IVU Search for the Cause of UTI • Anatomical abnormalities: urinary tract obstruction, nephrolithiasis, vesico-ureteral reflux • Functional disturbances: Voiding dysfunction Traditional goals of performing imaging in a child with UTI to detect urologic abnormalities: VUR, obstructive uropathy, bladder dysfunction to detect renal parenchymal damage Imaging studies in children with UTI Renal ultrasonography (RUS) Voiding cystourethrography (VCUG) Radionuclide cystography ( RNC) Scintigraphic rénal imaging (DTPA,DMSA) Advantages and disadvantages of RUS 1- RUS primarily provides an anatomic evaluation and is used to seen renal anomalies and hydronephrosis, renal parenchymal abnormalities, urethral dilatation bladder wall thickening ,ureterocells or calculi 2-RUS is not sensitive for focal or general scarring 3- Normal RUS dose not exclude VUR. RNG: VCUG or RNG? 1- lower radiation dose 2- Continuous monitoring during study for reflux 3- Dose not provide any anatomic evaulation of bladder or urethra 4- Reflux grading is not accurate Grading of reflux International classification of vesicoureteral reflux Grades of Reflux VUR is benign(1) • • Natural tendency of VUR to resolve spontaneously The historical studies showing that VUR is much more common, even among healthy children, • Evidence supporting the role VUR leading to pyelonephritis is controversial The unanimous conclusion of recent meta-analyses on the treatment of VUR has been that surgical abolishment of VUR, compared with microbial UTI prophylaxis and spontaneous resolution of VUR, has the same risk of new renal parenchymal injury or recurrent non-febrile UTI. • VUR is benign(12) • The antimicrobial prophylaxis of recurrent UTI is controversial too, and it may have unpleasant short-term side effects and increase the antimicrobial resistance of bacteria • In one randomised prospective study comparing continuous, intermittent or no treatment with antimicrobials in children with VUR, there was no difference between the groups studied in the risk of recurrent UTI or renal parenchymal injury. Conclusions: Vesicoureteral reflux is a fairly common phenomenon that can be associated with congenital renal dysplasia.Vesicoureteral reflux does not markedly increase the risk of recurring UTI or new acquired renal scars. The surgical correction of VUR does not prevent recurrences of nonfebrile UTI or new renal scars. In some children VUR is a symptom of developmental maturation defect of the “uretero-vesical valve. VUR is not benign • VUR predisposes to UTI and renal scars • There is not an age limit for renal scarring • Scarring can be prevented VUR is not benign Conclusion I believe it may be possible to reduce the rate and extent of renal scarring in future by altering our approach to infant and childhood UTIs, with more prompt diagnosis and treatment and an awareness of the potential hazard that having VUR may cause in this setting. The hope is, that by doing this, we will reduce the numbers of adults with hypertension and renal failure in the next generation of adults. Treatment of UTI • First: empiric treatment • Then: according to the result of culture Treatment of Pyelonephritis • Completely intravenous treatment • Initial 3-4 days IV treatment followed by oral treatment • Completely oral treatment (except high risk children) Indications for hospitalization • • • • • Age <2 months Clinical urosepsis or potential bacteremia Immunocompromised patient Vomiting or inability to tolerate oral medication Lack of adequate outpatient follow-up (eg, no telephone, live far from hospital, etc.) • Failure to respond to outpatient therapy