Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
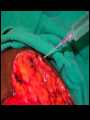
Wound Healing Wound Care Saran Worasakwutiphong MD. WOUND CARE • Most wounds heal with minimal intervention. • Systemic diseases, hospitalized • Nonhealing • 3 types : –(a) acute wound –(b) wound-healing difficulties –(c) chronic wound • Basics of wound care treat the broad spectrum of wounds • Understanding the biochemical and cellular aspects of tissue repair • Maximizing rates of limb salvage • Choosing a wound-care modality • Tetanus prophylaxis • History and physical examination • cause of the wound • identifying any comorbid conditions • Systemic & local factors • interfere healing • Bioburden 1. Contaminated (without proliferation) 2. Colonized (multiplying without reaction) 3. Critically colonized (host resistance is beginning) 4. Infected (expanding bacterial host reaction) • Wound cleansers – colonized and contaminated wounds • Surface irrigation with saline – contaminated wounds • Surgical debridement – infected wounds Most wounds: Antibiotics = unnecessary Antibiotic therapy • • • • Cellulitis Contaminated wounds (oral flora, animal bites) Mechanical implants Infected wounds • Healing decreases • Increased pain • straw-colored “oozing” from the skin Wound Bed Preparation T I M E •issue debridement •nfection control •oisture wound 13 Healing by reducing the bioburden Remove eschar - matrix formed from exudated serum Prolong inflammatory stage of wound healing Persistent bacterial colonization Meal for bacteria • • • • • • • Surgical Enzymatic Mechanical Autolytic Water jet Syringe with a 20-gauge 15 psi Maggot Sharp Debridement Moisture ADJUNCTS TO WOUND TREATMENT Debridement Dressings Negative-Pressure Wound Therapy Hyperbaric Oxygen Growth Factors Skin Substitutes Wound dressing Wound characteristics & treatment goals Films for incisions Hydrogels or hydrocolloids for open wounds Light exudates - Hydrogels, films Moderate exudates - Hydrocolloids Heavier exudate - Alginates, foams, NPWT Necrotic tissue - Surgical debridement Antiseptic GAUZE • • • • Traditional first choice Moist to dry dressings Traumatic and proinflammatory Expenses, painful, nonselective debriders, damage to healthy tissue, leave behind fine microfibers • Small, noncomplicated wounds • Impregnated with petrolatum, iodinated compounds, keeping moist Impregnated Gauze Bactrigas Urgotul • Impermeable to fluids, passage of small gas • Combination with gauze to maintain the moisture • Cover and protect freshly closed incisions and skin graft donor sites enhance epithelialization • Should not be used in contaminated / fragile skin prone to tearing Film Transparent Dressing • Maintaining a moist wound • Rehydrating wounds • Autolytic debridement • Absorb moderate amounts of fluid • Can be used in infected wounds • Nonadhesive, minimal pain • Pastes, powders, or sheets • Form an occlusive barrier & absorbs mild exudates • Left on the wound for 3 to 5 days • Not to be used in heavily colonized with bacteria,esp. anaerobes • Nonadhering polyurethane • Occlusive cover • Useful in highly exudative wounds • • • • • • Brown seaweed Useful in wounds with heavier exudate Frees from the multiple dressing changes Not to be used in nonexudative wounds Absorb ~20 times in fluid Should be covered with a semiocclusive dressing 36 Most beneficial = Silver Broad spectrum of microbicidal with low toxicity to human cells cell membrane permeabilizer inhibitor of cellular respiration nucleic acid denaturer Also against vancomycin-resistant Enterococcus(VRE) Methicillin-resistant Staphylococcus aureus(MRSA) Silver Sulfadizine 38 Silversulfadizine Cream 39 • Cadexomer iodine : slow-release form of iodine formulated bactericidal levels • Silver sulfadiazine • Mupirocin • Topical antibiotics • • • • Neomycin Gentamicin Metronidazole Bacitracin ointments and creams. Topical Antibiotic 41 1. Porous sponge within the wound 2. Covered by an airtight occlusive film 3. Vacuum system • • • • Relief of edema diffusion O2 to cells Removes deleterious enzymes Remove excess exudate Wound contraction Sponge should not be placed on normal skin, sensitive to pressure and ischemia Optimally pressure ~ 125 mm Hg Lymphatic leaks, venous ulcers, DM, fistulae, sternal wounds, orthopedic wounds, and abdominal wounds Contraindications Malignancy Ischemia Inadequately debrided / badly infected wounds VAC dressing • 100% O2 saturation at 2 to 3 ATA • O2 saturation plasma 0.3% to 7% • Periwound area/extremity rise in tcPO2 when supplemental O2 • Not benefit: – normal environmental perfusion – ischemic limbs who need a bypass • Still a paucity of RCT to support its use Hyperbaric Oxygen • Platelet-derived growth factor (PDGF) – Becaplermin (Regranex) • Vascular endothelial growth factor (VEGF) clinical trials • Diabetic foot, irradiated wounds and in aged. • Only in a well-prepared wound bed Digest necrotic, devitalized tissue and prevent slough and eschar Sometimes associated with pain Less traumatic < surgical debridement Papain with urea Proteases Collagenase • • • • • • Tissue-engineered products Contain living cells that are cellular factories Applied to meticulously clean wounds Adequate vascularity Immobilized useful for sites prone to contracture (neck, axillae) 53 54 • • • • • • • Silicone sheets increased moisture & collagenolysis Steroids Pressure garments Calcium channel blockers Topical salicylic acid • Silicone sheets improves the appearance of scars • increased moisture & • collagenolysis • Steroids • Pressure garments. • Calcium channel blockers • Topical salicylic acid Nutrition Nutrition DIRTY OPEN WOUND CLEAN OPEN WOUND CLOSE WOUND Secondary Intention Primary Closure Skin Graft