Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
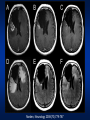
Antiangiogenics as Chemosensitizers: Out of the Frying Pan into the Fire? Dr. Urban Emmenegger Potential Conflict of Interest • Consultant / 2008 – – Amgen • Research Grant – Consultant / 2007 – – Novartis • Research Grant / 2007 – – Wyeth Montreal March 27 & 28, 2009 1st Quebec Conference on Therapeutic Resistance in Cancer Antiangiogenics as Chemosensitizers: Out of the Frying Pan into the Fire? Urban Emmenegger, MD Clinician-Scientist Sunnybrook Odette Cancer Centre & Research Institute Sunnybrook Health Sciences Centre Department of Medicine, University of Toronto 2075 Bayview Avenue, Toronto/ON M4N 3M5, Canada [email protected] Disclosure Consulting Fees: Amgen, Novartis Research Funding: Novartis, Wyeth Acknowledgements Sunnybrook Research Institute Sunnybrook Odette Cancer Centre Annabelle Chow Scott Berry Edward Chow Yoo-Joung Ko Linda Rabeneck Maureen Trudeau Bob Kerbel John Ebos Giulio Francia Christina Lee Tony Mutsaers Terence Tang William Cruz Chris Folkins Kae Hashimoto Shan Man Yuval Shaked Ping Xu University of Pisa, Pisa/Italy Guido Bocci D. Dumont M. Julius Objectives 1) To review basic principles of tumor angiogenesis and antiangiogenic therapies. 2) To discuss the rationale for combining chemotherapy with antiangiogenic agents as a means to overcome/delay resistance. 3) To identify challenges of this approach. Hippocrates… noticed that blood vessels around a malignant tumor looked like the claws of a crab. He named the disease karkinos (the Greek name for crab) … (http://medicineworld.org/cancer/history.html) Tumor angiogenesis: therapeutic implications Folkman J. N Engl J Med. 1971;285(21):1182-6 TAF inhibition reverses this process 3 1 2 Local (sprouting) angiogenesis Sex hormones IL-8 PDGFs VEGF-B EGF PlGF FGFs Thrombospondin-1/2 Interferon-α PEDF Angiostatin Endostatin Vasostatin Tumstatin Canstatin Arresten … VEGF-C VEGF-A VEGF-D angiogenesis angiogenesis angiogenesis angiogenesis angiogenesis The VEGF Family And Its Receptors PlGF VEGF-A* 206 VEGF-B 189 165 121 VEGFR-2 (Flk-1/KDR) VEGFR-1 VEGF-C VEGF-D VEGFR-3 (Flt-4) (Flt-1) Angiogenesis ‘Inflammation’ *VEGF-A = ‘VEGF’ Angiogenesis Lymphangiogenesis Lymphangiogenesis endothelial cell ‘Systemic’ angiogenesis (i.e., vasculogenesis) Kerbel RS. N Engl J Med 2008;358:2039-2049 Agents Targeting the VEGF Pathway Anti-VEGF antibodies Soluble decoy VEGF receptors VEGF (Bevacizumab) (VEGF-Trap) mTOR inhibitors (Temsirolimus, Everolimus) P P P P P P VEGFR-1 P P AntiVEGFR antibodies (IMC-1121b) VEGFR-2 endothelial cell Small-molecule VEGFR kinase inhibitors (Sunitinib, Sorafenib, Axitinib, Cediranib … ) Sunitinib VEGFR1-3 PDGFR alpha PDGFR beta RET KIT FLT-3 Sorafenib VEGFR1-3 C-/B-RAF PDGFR beta RET KIT FLT-3 http://www.kinomescan.com/show_data.asp Vatalanib Delta-like Ligand 4 - Notch Pathway Increased angiogenesis: functionally abnormal+++ vasculature Decreased angiogenesis: vascular rarefaction reduced blood flow, severe hypoxia reduced blood flow, severe hypoxia Adapted from Hicklin DJ. Nature Biotechnology 25, 300 - 302 (2007) ‘Accidental’ Anti-Vascular Agents • • • • • • • • • • • • • chemotherapeutics hormonal therapies radiation therapy COX-2 inhibitors corticosteroids thalidomide LMW heparins ACE inhibitors propranolol glitazones doxycyclin valproic acid ... Léauté-Labrèze C, N Engl J Med. 2008;358(24):2649-51. Antiangiogenic Therapies: Phase III Success Stories 2004 2006 Non-small cell lung cancer: Bev + PC (PFS/OS) 2007 1971 Folkman Hypothesis 1983/89 VPF/VEGF 1997 Bevacizumab Colorectal Cancer: Bev + FOLFOX (PFS/OS) Breast Cancer: Bev + Paclitaxel (PFS) Renal Cell Cancer: Sunitinib (PFS/OS) Sorafenib (PFS) Temsirolimus (PFS/OS) Bev + IFN-alfa 2a (PFS) 2008 Hepatocellular Ca: Sorafenib (PFS/OS) Renal Cell Cancer: Everolimus (PFS) Activity of Single-Agent Bevacizumab Tumor Type (Ref) Objective SD RR (%) (%) PFS/TTP (median, m) Comments 0 - 4 Phase II, n=15, 10 mg/kg q2wks 6.7 16 5.6 Phase I/II, n=75, 3-10-20 mg/kg q2wks 10 - 4.8 Phase II, n=39, 10 mg/kg q2wks 5 20 5 Phase II, n=46, 10 mg/kg q2wks Recurrent Ovarian Ca (Burger 05) 18 55 - Phase II, n=62, 15 mg/kg q3wks Colorectal Ca (2nd line) (Giantonio 07) 3.3 - 2.7 Phase III, n=243, 10 mg/kg q2wks 0 - 3 Phase II, n=5, 15 mg/kg q2wks CR Prostate Ca (Reese 01) Met Breast Ca (Cobleigh 03) Kidney Ca (Yang 03) Recurrent NHL (Stopeck 05) Metastatic Melanoma (Varker 07) Activity of Bevacizumab & Chemotherapy Ref Hurwitz mCRC 1st line Giantonio mCRC 2nd line Sandler NSCLC 1st line Miller ABC 1st line Tx IFL +B IFL FOLFOX4+B FOLFOX4 P-C +B P-C P +B P Median Survival (m) 20.3 15.6 12.9 10.8 12.3 10.3 26.7* 25.2* 1y survival (%) 74.3 63.4 - - 51 44 - - Median PFS (m) 10.6 6.2 7.3 4.7 6.2 4.5 11.8 5.9 Overall RR (%) 44.8 34.8 22.7 8.6 35 15 36.9 21.2 mCRC = metastatic colorectal cancer, NSCLC = non-small cell lung cancer, ABC = advanced breast cancer, IFL = irinotecan-fluorouracil-leucovorin, FOLFOX4 = oxaliplatin-fluorouracil-leucovorin, P = paclitaxel, C = carboplatin , B = bevacizumab Underestimation of the true potential? • Antiangiogenics developed without biomarker guidance for optimal dosing: – flat dosing common for RTKIs – various bevacizumab regimens • Lack of markers for patient selection • Challenging integration into current standards of care Rationale against Combination Therapy • Antivascular effects I – inhibition of neo-angiogenesis – induction of endothelial cell apoptosis – impaired mobilization of CEPs and other bone marrow derived cells – vasoconstriction de Bazelaire, C. Clin Can Res 2008;14:5548-5554 reduced blood flow → decreased pO2 and nutrients availability, low pH → ANTAGONISM: reduced chemotherapy deposition, diminished cytotoxic activity drug Rationale for Combination Therapy • Antivascular effects I – inhibition of neo-angiogenesis – induction of endothelial cell apoptosis – impaired mobilization of CEPs and other bone marrow derived cells – vasoconstriction de Bazelaire, C. Clin Can Res 2008;14:5548-5554 reduced blood flow → decreased pO2 and nutrients availability, low pH → SYNERGISM: impaired tumor cell repopulation Rationale for Combination Therapy • Antivascular effects II – vascular ‘normalization’ Science 2005(307):58 – 62; Mol Can Ther 2008(7):3670-84 Rationale for Combination Therapy • Antivascular effects III – disruption of ‘vascular niche’ → diminished cancer stem cell compartment – impaired mobilization of CEPs and other bone marrow derived cells → impaired vascular repair → augmentation of chemotherapyrelated antivascular effects Tumor Angiogenesis versus Physiological Angiogenesis Antivascular effects Plasma concentration of cytotoxic drug Conventional (MTD) Chemotherapy Tumor cell cytotoxicity Vascular repair Antivascular effects 3 weeks Vascular repair Antivascular effects 3 weeks Shaked et al. Cancer Cell. 2008;14(3):263-73. Bertolini et al. Nat Rev Cancer. 2006;6(11):835-45. Tumor cell cytotoxicity Myelosuppression Antiangiogenesis Antivascular effects Plasma concentration of cytotoxic drug Metronomic Chemotherapy 3 weeks 3 weeks Kerbel RS, Kamen BA. Nat Rev Cancer. 2004;4(6):423-36. Emmenegger U, Kerbel RS. Onkologie. 2007;30:606-608. VEGF Targeting Agents: Beyond Antivascular Effects • Direct anti-tumor effects • Immunomodulatory effects • Mitigation of ‘cancer-associated systemic syndrome’ Xue et al PNAS 2008 105:18513-518 Anti-VEGF agents confer survival advantages to tumor-bearing mice by improving cancer-associated systemic syndrome Clinical Applications: Challenges • phase III failures • pancreatic cancer: Bev + Gemcitabine • breast cancer: Bev + Capecitabine • colorectal cancer: Vatalanib + FOLFOX (1st and 2nd line) • diminished PFS/OS benefit in ‘2nd generation’ trials • > 50 agent(s) in clinical development • concurrent/sequential use? • continuous/intermittent use? • small molecule drugs or antibodies? • costs • side-effects • course of action in case of tumor progression? • intrinsic or acquired resistance Mancuso et al. JCI 2006;116:2610–2621 Grothey et al. JCO 2008;26:5326-5334 Resistance to Antiangiogenic (Mono-)Therapy Vascular Remodeling Evasive Resistance Co-option Reduced Vascular Dependence Norden, Neurology 2008(70):779-787 Dissociation of antiangiogenic and anti-tumor effects NS: 1 week LDM CPA: 1 week LDM CPA: relapse NS: 4 weeks Emmenegger Cancer Res 66;1664-1674 (2006) Reduced vascular dependence Hypoxia, Starvation Acute survival Proliferation Cytostasis • Autophagy Cell death ~ • Necrosis • Apoptosis • Autophagy dual function ‘Macro-Autophagy’ ‘Stress’ Step Initiation Structure Sequestration Autophagosome formation & maturation Phagophore Autophagosome Molecules Involved mTOR Beclin1 (Atg6) LC3 (Atg8) UVRAG Atg5 PI3kinase III Atg12 Atg9 Modifiers mTOR 3-methyladenine inhibitors → autophagy → autophagy inhibition stimulation Docking & fusion with lysosome Lysosome Vesicle breakdown, degradation of content, release of degradation products Autolysosome Cathepsins Chloroquine Bafilomycin A1 → autophagy inhibition As a consequence of metabolic or treatment-related stress, autophagy is initiated and proceeds stepwise. Schematic presentation of the various steps of the autophagic cascade, the structures formed, important molecules involved and pharmacological modifiers of autophagy. Reduced vascular dependence: a consequence of impaired autophagy? PC-3 standard culture conditions 2% PC-3 metabolic stress 19.47% LCR1.1 0.43% LCR1.1 5.26% Promotion of tumor progression by antiangiogenic therapy? Accelerated metastasis after short-term treatment with a potent inhibitor of tumor angiogenesis. Ebos JM, Lee CR, Cruz-Munoz W, Bjarnason GA, Christensen JG, Kerbel RS. Cancer Cell. 2009 Mar 3;15(3):232-9. Antiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasis. Pàez-Ribes M, Allen E, Hudock J, Takeda T, Okuyama H, Viñals F, Inoue M, Bergers G, Hanahan D, Casanovas O. Cancer Cell. 2009 Mar 3;15(3):220-31. i.v. tumor implantation (LM2-4LUC+ Cells) Vehicle Group A Group B Group C 120 mg/kg 120 mg/kg Days Post Tumor Implantation Group A 1 2 Tumor Burden (Photons/s) 10 8 3 4 5 Group B 6 7 1 2 3 4 5 Group C 6 7 1 2 3 4 5 7 10 7 21 10 6 27 -7 0 7 14 21 Days Postimplantation 30 28 35 42 6 7 Loges et al. Silencing or fueling metastasis with VEGF inhibitors: antiangiogenesis revisited. Cancer Cell. 2009;15(3):167-70. Conclusions I • Antiangiogenic therapy is a clinical reality! • Angiogenesis is a highly regulated process. • Although the tumor vasculature is morphologically and functionally aberrant, common regulatory mechanisms remain intact and represent promising treatment targets. • Antiangiogenic agents can potentiate the antitumor effects of chemotherapeutics (and vice versa) but much remains to be learned to optimize the clinical benefit of such combinations. Conclusions II • The biological understanding of the process of tumor vascularization is rapidly evolving, but this is not yet matched by the way antiangiogenic agents are used in the clinic. • There is an unmet need for biomarkers in order to optimize dosing of antiangiogenics, and for the selection of patients most likely to benefit from such agents. • Various mechanisms of intrinsic or acquired resistance to antiangiogenic agents have been described. Conclusions III • Resistance to combinations of cytotoxic and antiangiogenic agents is less well characterized. • Stopping the administration of antiangiogenic agents at progression might facilitate tumor growth acceleration. • Novel findings suggest that antiangiogenic therapy might promote invasive tumor growth and metastatic disease progression. • Tumor promoting effects could explain the yet limited overall survival benefit resulting from the use of antiangiogenic agents and are of special concern in the (neo)adjuvant setting. ‘The greater our knowledge increases, the greater our ignorance unfolds.’ John F. Kennedy