Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
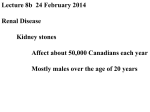
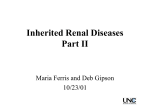
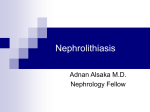
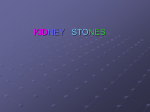
Nephrolithiasis Karen Estrella-Ramadan 07/06/12 The classic adult presentation of sudden, debilitating flank pain is uncommon in children. 50%: abdominal, flank, or pelvic pain (>in older children and adolescents) In infants may mimic colic, > vomiting In preschool-age children: as UTI 33%-90%: Gross or microscopic hematuria is found in 33% to 90% (equally across age groups) ◦ 3 samples (1 wk apart) with RBC > 5 Balance of stone-promoting and -inhibiting factors. Gillespie R S , Stapleton F B Pediatrics in Review 2004;25:131-139 ©2004 by American Academy of Pediatrics Increased Intestinal Calcium Absorption ◦ Vitamin D excess Renal Tubular Dysfunction ◦ Renal tubular phosphate leak ◦ Impaired renal tubular calcium absorption ◦ Type 1 (distal) renal tubular acidosis ◦ Dent disease ◦ Bartter syndrome Endocrine Disturbances ◦ Hypothyroidism ◦ Adrenocorticoid excess ◦ Hyperparathyroidism Bone Metabolism Disorders ◦ Immobilization ◦ Rickets ◦ Malignancies ◦ Juvenile rheumatoid arthritis Other ◦ Familial idiopathic hypercalciuria ◦ Drugs (certain diuretics, corticosteroids) ◦ Urinary tract infection ◦ Williams syndrome ◦ Increased renal prostaglandin E2 production ◦ Hypercalcemia ◦ Hypophosphatemia ◦ Glycogen storage disease Etiology 1. CALCIUM • Most children who have hypercalciuria and urolithiasis have normal serum calcium concentrations. 2. Infection > associated with Proteus, Providencia, Klebsiella, Pseudomonas, Enterococci ◦ Urease producers ◦ Highly favorable for struvite (magnesium ammonium phosphate) stone formation 3. Uric acid Few childhood stones are composed purely of uric acid. Uric acid excretion is highest in infancy and remains high, relative to adult values, until adolescence. Normal levels of urinary uric acid are so high in infants that crystals may precipitate in diapers and be misidentified as blood. 3.Hyperoxaluria and Oxalosis Primary hyperoxalurias types I and II: rare autosomal recessive ◦ includes nephrocalcinosis and nephrolithiasis ◦ Growth failure, malnutrition, uremia Secondary hyperoxaluria: sec to excessive intake of oxalate precursors (ethylene glycol, ascorbic acid), increased absorption of oxalate (IBD, extensive bowel resection), or deficiency of cofactors in oxalate metabolism (pyridoxine deficiency) ◦ Oxalosis develops as calcium oxalate precipitates in multiple organs and joints. ◦ Oxalate deposition in the kidneys impairs renal function, further elevating serum oxalate levels. 4. Cystinuria Autosomal recessive disorder of renal tubular transport ◦ excessive excretion of cystine, arginine, lysine, and ornithine. Other Causes CF: sec to hypercalciuria, hyperoxaluria, and hypocitraturia Drugs: TMP-SMX and ceftazidime , protease inhibitors (indinavir), furosemide, acetazolamide, and allopurinol An important emerging cause of childhood stones is the ketogenic diet, with an incidence of urologic stones as high as 10%. Used for refractory seizures ◦ A high-protein, low-carbohydrate, low-fluid dietary regimen is associated with hypercalciuria, hyperuricosuria, hypocitraturia, and low urine volume. CBC, CMP, uric acid Gillespie R S , Stapleton F B Pediatrics in Review 2004;25:131-139 ©2004 by American Academy of Pediatrics Hypoechoic shadow Renal calculus on unenhanced computed tomography (CT). Gillespie R S , Stapleton F B Pediatrics in Review 2004;25:131-139 ©2004 by American Academy of Pediatrics Labs Complete metabolic evaluation: ◦ Pt at home, consuming regular diet and with no infection. ◦ ideally get 24hrs urine collection, but due that is difficult, new standards for single collections Further workup if no stone or + calcium oxalate: ◦ Cystine levels (urine) in 1st specimen ◦ PTH: if hypercalciuria, hypercalcemia, hypoP ◦ Vitamin D levels Treatment Goals: Prevent additional renal damage Manage pain Expedite passage or removal of any stones Prevent new stones from forming. Conservative Increase water intake Analgesics: ◦ Mild: NSAIDS (stop 3 days before sx procedure) ◦ Moderate: Tylenol + codeine ◦ Severe: Morphine *in cases of distal: may use doxazosin (alpha blocker) Abx: if + urine cx Peds Urology referral Stone Removal • <5mm stones will pass without further tx Intervene if: signs of infection, complete obstruction, partial obstruction by a stone in a solitary kidney, renal insufficiency, or if the stone is greater than 5 mm in diameter, as it is unlikely to pass spontaneously. Options: 1. Extracorporeal shock wave lithotripsy (ESWL) < 1cm on pelvis 2. Percutaneous nephrostolithotomy (PCNL) > 2 cm, harder stones: calcium, cystine, structural anormalities 3. Ureteroscopy In Ureter or bigger (struvite) Treatment specific 1. Hypercalciuria: ◦ Good hydration + a low-sodium diet ◦ If doesn’t work: Thiazide diuretics (stimulating calcium reabsorption in the distal tubule) ◦ Patients should avoid vitamin D supplements. ◦ Citrate supplementation helps prevent stones in patients who have renal tubular acidosis or hypocitraturia. ◦ Avoid high protein diet (increase calcium excretion) ◦ High K diet 2. Hyperoxaluria Decrease Na intake Avoid: ◦ As vitamic C and D ? Supplemental: citrate, Mg, P Increase calcium intake Diuretics: hydrochlorothiazide Combined liver and kidney transplantation remains the only definitive therapy. 3. Uric Acid Decrease Na intake- may decrease urinary uric acid (and calcium) excretion. If fails: base supplementation with citrate or bicarbonate may be indicated. ◦ Alkaline urine= > solubility of uric acid ◦ Allopurinol 4. Cystine: Hydration + urine alkalinization Refractory: D-penicillamine, tiopronin, and alpha-mercaptopropionylglycine (bind cystine) References http://pedsinreview.aappublications.org/c ontent/25/4/131.full.pdf+html http://pednephrology.stanford.edu/secure /documents/Nephrolithiasis-Children.pdf http://emedicine.medscape.com/article/9 83884-treatment#a1156