Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
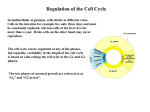
CRITICAL APPRAISAL Bob Lightowlers Mitochondrial Research Group Institute of Neuroscience NOT EVERYTHING THAT IS PUBLISHED IS CORRECT!! NOT EVERYTHING THAT IS PUBLISHED IS CORRECT!! ONLY 15% OF PUBLICATIONS ARE TRUSTWORTHY NOT EVERYTHING THAT IS PUBLISHED IS CORRECT!! ONLY 15% OF PUBLICATIONS ARE TRUSTWORTHY GUILTY UNTIL PROVEN INNOCENT Mutations in mitochondrial cytochrome c oxidase genes segregate with late-onset Alzheimer Disease Hypothesis: Alzheimers Disease could be caused by defects in activity of the respiratory chain complex cytochrome c oxidase Why ? • Lack of FH is a negative risk factor Why ? • Lack of FH is a negative risk factor • Risk of AD increases with affected maternal relative (mtDNA?) Human mtDNA • An autosomally replicating genome • Found in mitochondrial matrix • Circular genome with short (1.2knt) noncoding region (D-loop) 16,569 bp • Comprises app. 0.1% of total cell DNA • Varies enormously in copy number/cell Approx. 700 in fibroblasts to >200,000 in some mammalian oocytes • Maternally inherited • Often heteroplasmic in the diseased state Why ? • Lack of FH is a negative risk factor • Risk of AD increases with affected maternal relative (mtDNA?) • Mutations in mtDNA can lead to defective OXPHOS Why ? • Lack of FH is a negative risk factor • Risk of AD increases with affected maternal relative (mtDNA?) • Mutations in mtDNA can lead to defective OXPHOS • Neurons may be particularly susceptible to such defects Why ? • Lack of FH is a negative risk factor • • Risk of AD increases with affected maternal relative (mtDNA?) • Mutations in mtDNA can lead to defective OXPHOS • Neurons may be particularly susceptible to such defects • COX activity reported to decrease in brain of AD patients Methods used • MtDNA isolation and sequencing in patients, asymptomatic relatives and controls Methods used • MtDNA isolation and sequencing in patients, asymptomatic relatives and controls • All three COX genes sequenced Methods used • MtDNA isolation and sequencing in patients, asymptomatic relatives and controls • All three COX genes sequenced • Quantification of mutations in all samples Methods used • MtDNA isolation and sequencing in patients, asymptomatic relatives and controls • All three COX genes sequenced • Quantification of mutations in all samples • Platelet fusion from AD patients to neuronal cells lacking mtDNA (rho0) Generation of transmitochondrial cybrids EthBr Biopsy Enucleation Methods used • MtDNA isolation and sequencing in patients, asymptomatic relatives and controls • All three COX genes sequenced • Quantification of mutations in all samples • Platelet fusion from AD patients to neuronal cells lacking mtDNA (rho0) • Analysis of respiratory enzyme activity in the cybrids Methods used • MtDNA isolation and sequencing in patients, asymptomatic relatives and controls • All three COX genes sequenced • Quantification of mutations in all samples • Platelet fusion from AD patients to neuronal cells lacking mtDNA (rho0) • Analysis of respiratory enzyme activity in the cybrids • Analysis of ROS production in cybrids Results 506 Patients and 95 controls Results 506 Patients and 95 controls 10 clones of all three COX genes sequence Results 506 Patients and 95 controls 10 clones of all three COX genes sequence 6 mutations found in COI and COII Results 506 Patients and 95 controls 10 clones of all three COX genes sequence 6 mutations found in COI and COII Different levels of heteroplasmy but levels significantly greater in the AD cohort Results 506 Patients and 95 controls 10 clones of all three COX genes sequence 6 mutations found in COI and COII Different levels of heteroplasmy but levels significantly greater in the AD cohort No disease-associated mutations in COIII gene Results 506 Patients and 95 controls 10 clones of all three COX genes sequence 6 mutations found in COI and COII Different levels of heteroplasmy but levels significantly greater in the AD cohort No disease-associated mutations in COIII gene AD cybrids but not controls had low COX activity Results 506 Patients and 95 controls 10 clones of all three COX genes sequence 6 mutations found in COI and COII Different levels of heteroplasmy but levels significantly greater in the AD cohort No disease-associated mutations in COIII gene AD cybrids but not controls had low COX activity Increased production of ROS in AD cybrids Critical evaluation: How appropriate and robust are the methods ? Is the data (and evaluation) robust ? Are the conclusions valid, based on the reported data ? How often do the authors refer to themselves ? How does the paper stand the test of time ? Is there any conflict of interest ?