Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
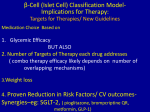
Diagnosing Diabetes In Adults– Type 1, LADA, or Type 2? Part 3 Stanley Schwartz MD, FACE, FACP Affiliate Main Line Health Emeritus, Clinical Assoc. Prof. of Medicine Perlman School of Medicine, University of Pennsylvania Struan F.A. Grant, Ph.D Children’s Hospital of Philadelphia Associate Professor, University of Pennsylvania Vanessa Guy Children’s Hospital of Philadelphia Senior Clinical Research Coordinator Co-Investigators NIH RO-1, Genes in LADA New β-Cell Centric Construct: Implications Insulin Resistance Exposes and Exacerbates the Core β-Cell Defect Genetically- Based Exacerbated by Environmental issues- Diet, Activity, Biome Includes Brain-Directed, Peripheral Insulin Resistance Loss of Dopa- Surge in SCN IR Impairs β-Cell Function by: • Lipo and gluco-toxicity • Inflammatory Mechanisms • Adipocytokine effect on β-cell IR is NOT a Core Defect (as only ~1/3 of IR patients have Diabetes) (but CLEARLY, IR is a focus of therapy in patients with vulnerable β-cells) Simplistic Inflammatory and Non-Inflammatory Effects of Insulin Resistance IAPP boosts islet macrophage IL-1 in type 2 diabetes : Nature ...www.nature.com Multiple Causes IRMultiple Potential Therapies Weight Reduction Biome ProIR Biotics, Pre-Biotics Central IR/ Appetite Peripheral IR TZD (Pio-) , Metformin Bromocriptine-QR Inflammation IR AntiInflam. New β-Cell Centric Construct: Implications Environmental Risk Factors in T1D/T2D, ? ‘LADA’ T1D Seasonality at diagnosis Migrants assume risk of host country Risk factors from case-control studies • • • • • Hormones • Vitamin D Stress • Cow’s Milk Improved Hygiene • Gut-microbial Balance – Biome Infant/childhood diet • Lack of Physical Activity Viruses – exposures as early as in utero T2D LADA Obesity-Diet Coffee More Educated Lack of Physical Activity AGE ingestion Going Forward: New Focus of Care: Primary Prevention: ? For All DM in New Classification Genetic / antibody screening 1 effort to identify eligible subjects Potential Immune Modulators 2 Environmental Modulation 3 – Especially as we learn morevaccination, endocrine disruptors, diet, exercise Intervention needs to be 2 extremely safe Defining risk factors will facilitate primary prevention studies Atkinson, Eisenbarth,THE LANCET • Vol 358 • July 21, 2001 225 1 3 APPLY MODEL TO ALL DM New β-Cell Centric Construct: Implications Diagnosis Markers By Virtue of Family History ‘DM”, Physiogomy, hyperglycemia in Prediabetic and diabetic range Genes • Family History • Genotype- HLA, TCF7L2, etc β-Cell • FBS, 2hr ppg, HgA1c, ? C-peptide, ?other Inflammation • Antibodies, Inflammatory Markers, T-Cell function, ?other Insulin Resistance • BMI, Adiponectin, Adipocytokines, ? Other Abilities to get what/which above data will be cost-dependenteach patient, insurers, formulary, government Current Terminology Should Reflect the β-Cell Centric Approach; or,…we need to Develop a New Terminology Older Younger ‘LADA’ T2D MODY, monogenic T1D SPIDDM Autoimmune T2D T2D +,which +,which +,which +,which + + + +/- Genes - mono +,which - poly +,which Inflammation +/- Resistance +/- +/- ─ +/- +/- +,which +,which +,which +,which +,which Environment ─ Implications for Therapy β-Cell (Islet Cell) Classification ModelImplications for Therapy: (Not Core Defects)-Targets for Therapies GIVES US ‘PERMISSION’ TO USE ANY LOGICAL THERAPY for ANY DIABETIC ‘TYPE” Egregious Eleven 1. 2. 3. 4. β-CELL α cell Glucagon defect ↓ INCRETIN EFFECT-Incretin Inflammation 5. Liver 6. Muscle 7. Fat 8. Kidney 9. Brain 10. Stomach/Intestine 11. Colon- Biome With Appropriate , on bent-knee, thanks and appreciation, to my (Renal fellow when I was an intern) friend and collaborator, Dr. Ralph DeFronzo β-Cell (Islet Cell) Classification ModelImplications for Therapy: Egregious Eleven 1. β- Cell 2. α- Cell 3. Incretin 4. Inflammation inflammation 5. Liver 6. Muscle 7. Fat 8. Kidney 9. Brain 10. Stomach/Intestine 11. Colon/Biome BRAIN Gene(s) ↑Appetite SCN INSURES it’s GETTING ENOUGH GLUCOSE TO WORK!! Cells ‘complain’ not getting enough glucose ↓Dopa surge Inflammation Insulin resistance Lipotoxicity Gene/ Envir interAction!! Environment ↑Glucagon ↓ Amylin ↓ Incretin effect ↑ GLP-1 resistance ↓ β-Cell function ↓ β-Cell mass ↓Insulin PPG-HYPERGLYCEMIA Glucotoxicity β-Cell Centric Construct For Pathogenesis of All Diabetes: Implications for RX- EGREGIOUS ELEVEN CORE ISSUES Teach CROSSTALK BRAIN Gene(s) ↑Appetite SCN INSURES it’s GETTING ENOUGH GLUCOSE TO WORK!! Cells ‘complain’ not getting enough glucose ↓Dopa surge Inflammation Fat Liver Muscle Insulin resistance Lipotoxicity Gene/ Envir interAction!! Environment ↑Glucagon ↓ Amylin ↓ Incretin effect ↑ GLP-1 resistance ↓ β-Cell function ↓ β-Cell mass ↓Insulin PPG-HYPERGLYCEMIA Glucotoxicity β-Cell Centric Construct For Pathogenesis of All Diabetes: Implications for RX- EGREGIOUS ELEVEN CORE + IR ISSUES BRAIN ↑Appetite SCN Gene(s) INSURES it’s GETTING ENOUGH GLUCOSE TO WORK!! Cells ‘complain’ not getting enough glucose ↓Dopa surge Inflammation Fat Liver Muscle Insulin resistance Lipotoxicity Gene/ Envir interAction!! ↑Glucagon Colon biome Environment ↓ Amylin ↓ Incretin effect ↑ GLP-1 resistance ↓ β-Cell function ↓ β-Cell mass ↓Insulin Stomach Fast emptying PPG-HYPERGLYCEMIA Glucotoxicity Up-regulates SGLT-2 β-Cell Centric Construct For Pathogenesis of All Diabetes: Implications for RX- EGREGIOUS ELEVEN Kidney ALL ISSUES