Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
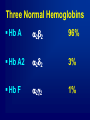
Points to be discussed: Definitions Patho-physiology Signs & Symptoms Diagnosis Options of management. Complications Preventive measures Long term follow up of patients DEFINITIONS THALASSEMIA MAJOR THALASSEMIA INTERMEDIA THALASSEMIA MINOR, TRAIT, HETEROGENOUS 4 An example of inheritance: Marriage between two carriers Developmental expression of the globin chains Embryonic hemoglobins z2e2 a2e2 z2g2 Fetal hemoglobins a2g2 HbF Adult hemoglobins a2d2 HbA2 a2b2 HbA Three Normal Hemoglobins Hb A a 2b 2 96% Hb A2 a 2d 2 3% Hb F a 2g 2 1% b-THALASSAEMIA An abnormality associated with one b gene is called b-thal minor (bTm). An abnormality associated with two b genes is called b-thal major (bTM). b chain production may be decreased or absent resulting in excess free a chains. If production is decreased we refer to the phenotype as b+, if absent bo. HAEMATOLOGICAL PROFILE B T Minor Hb N-Dec RCC Inc (Marrow compensating for ineffective haematopoiesis MCV Dec MCH Dec Hypochromasia + Anisocytosis ++ (Microcytes) Poikilocytosis Target Cells+ Immature Forms Polychromasia Coarse basophilic stippling Mentzer: MCV --- --- = if <13 thal minor RBC >13 then iron deficiency Shine - Lal: (MCV)2 X MCH = if <1530 then thal minor >1530 then iron deficiency England- Frazer : MCV- (Hgb X 5)RBC- 3.4 = if negative : thal minor positive : iron def - Hb. ELECTROPHORESIS HbA: HbF: Present N-Slightly Inc (Only compensating for 1 chain) HbA2: Inc (4-5%, reason unknown but this feature is used diagnostically differentiating from bTM or a TM) b TM b0b0 – most severe – no b chain production. b0b+ - moderately severe – some b chain production. b+b+ - Increased HbF with normal or elevated HbA2 – there is remained HbA. Clinical severity varies accordingly. CLINICAL ASPECTS Hepatomegaly and splenomegaly. Chronic haemolysis that may be accompanied by gallstones, gout and icterus (jaundice). Not usually detected until 6 months of age. Excess iron from blood transfusions may lead to cardiac and hepatic problems. As with other haemolytic anaemias, more iron is absorbed from the gut exacerbating iron overload. Largely overcome by the use of Desferroxamine. HAEMATOLOGICAL PROFILE Hb Anisocytosis Dec +++ (Macrocytes, Microcytes) Poikilocytosis Target cells +++ Tear drops Schistocytosis Acanthocytes, Howell Jolly Bodies, Target Cells (post splenectomy) Immature Forms Polychromasia ++ Nucleated RBC +++ (bone marrow response) Blood Film - BTM • X-RAYS IN THAL. PTs TRANSFUSIONAL IRON OVERLOAD IN THALASSEMIA 120 Death 100 Cardiac Failure Hypoparathyroidism Iron (g) 80 Hypothyroidism 60 Diabetes 40 Hypogonadism Cardiac arrhythmia 20 Hepatic Fibrosis --> Cirrhosis 0 1 3 5 7 9 11 13 15 17 19 Age (years) Thalassemia Centre, Dept. of Pediatrics University of Turin, Italy IRON ACCUMULATION IN TRANSFUSION-DEPENDENT ANEMIAS Blood Transfusion 0.3-0.5 mg iron/kg/day In a 50 kg person 15-25 mg/day Iron Accumulation 13-24 mg/day Iron Excretion (Urine & Feces) 1-2mg/day Management Medical /Nursing management Social and Behavioral management Management of complications Compliance Medical Management Blood Transfusion-----Dr. Khawla Chelation Therapy---- Dr Ahmad Bone Marrow Transplant Gene Therapy TRANSFUSION CARE OF THE CHILD WITH THALASSEMIA MAJOR Red Blood Cell Transfusion: Transfusion ≥ Hb 9.0 g/dl Extended red cell genotype Match donor blood to ABO, rhesus and Kell filter or wash blood – (white cell depletion) Vaccinate with hepatitis B Pre-tX Bone Marrow Transplant HLA matched Donor Preparation of the patient Consider selection criteria Stem cells could be collected by: Bone Marrow Aspiration Peripheral apheresis Cord Blood When 24 COMPLICATIONS Cardiac Endocrine Hepatic Renal Skeletal Virus transmission Blood reactions. TRANSFUSIONAL IRON OVERLOAD IN THALASSEMIA 120 Death 100 Cardiac Failure Hypoparathyroidism Iron (g) 80 Hypothyroidism 60 Diabetes 40 Hypogonadism Cardiac arrhythmia 20 Hepatic Fibrosis --> Cirrhosis 0 1 3 5 7 9 11 13 15 17 19 Age (years) Thalassemia Centre, Dept. of Pediatrics University of Turin, Italy CROSS-SECTIONAL STUDY OF 342 PATIENTS IN THE NIH-SPONSORED THALASSEMIA CLINICAL RESEARCH NETWORK REGISTRY* 16-24 yr (n=93) 25+ yrs (n=129) Hypogonadism (req. meds) Diabetes Mellitus 41% 9% 62% 21% Thyroid Disease Hypoparathyroidism Cardiac Disease (req. meds) 8% 1% 5% 17% 9% Age Group 23% (30/128) Reference: Adapted from Cunningham, et al. Blood. Online Feb. 26, 2004 DOI 10.1182 B-THAL. INTERMEDIA THALASSEMIA MAJOR – SURVIVAL Prevention • Premarietal Screening • Prenatal diagnosis • Pre Implantation Genetic Diagnosis