Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
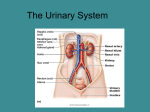
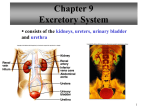
The Urinary System The Urinary System Urinary System – includes the paired kidneys and ureters and the single urethra Functions: • Excretion – the elimination of wastes and toxins from the body via urine (regulating water and ion balance and blood volume) • Hormone production – kidneys produce renin to regulate blood pressure and EPO to trigger erythropoiesis Figure 25.1a The Kidneys Kidneys – the functional organs of the urinary system, which are paired and retroperitoneal • Size: 12 cm length x 6 cm width • Mass – 150 g Figure 25.2 The Kidneys Fibrous capsule – the dense connective tissue layer giving the kidneys shape and support Renal hilum – the medial, concave indentation where blood vessels and ducts access the organs Figure 25.3b The Kidneys Kidney Layers: • Cortex - outer, lighter region where majority of filtration occurs • Medulla - inner, darker region of alternating renal pyramids and renal columns • Renal pyramids - a collection of collecting ducts that drain urine from the cortex • Renal column - tissue between pyramids where blood vessels pass to access the cortex Figure 25.3b The Kidneys Renal Papilla - bumpshaped structure at the tip of renal pyramid with pores that drain urine from the pyramids into the renal sinus Figure 25.3b The Kidneys Renal sinus - series of hollow spaces that collect urine and drain it into a ureter, includes the renal pelvis and calyces Figure 25.3 Nephrons Nephrons – functional units of the kidneys, acting as individual filters, numbering 1 million per kidney. Parts of a Nephron: • Glomerulus- porous capillary bed that leaks plasma and solutes, now called filtrate • Renal Tubule – highly folded passage that converts filtrate into urine Figure 25.4 Nephrons Parts of the renal tubule: • Glomerular (Bowman’s) capsule – start of the tubule that surrounds the glomerulus to catch its leaked fluids and solutes • Proximal convoluted tubule (PCT) – first coiled area in the cortex • Loop of Henle – long region that dips into medulla, includes descending and ascending limbs • Distal convoluted tubule (DCT) – second coiled area in the cortex Figure 25.4 Nephrons Collecting duct – tubule that collects urine from many nephrons for transport through a pyramid to the renal sinus Types of nephrons: Cortical – located higher in the cortex, only a small dip into the medulla Juxtamedullary – sit lower in the cortex, larger dip into the medulla Figure 25.5a Nephrons Other Nephron Capillaries – perform reabsorption of valuable nutrients from the filtrate, returning them to the plasma • Peritubular capillaries – surrounds the regions of the renal tubule in the cortex • Vasa recta – surrounds the regions of the renal tubule in the medulla Figure 25.5a Nephrons Glomerulus – bed of fenestrated capillaries surrounded by a glomerular capsule; together called a renal corpuscle • supplied by an afferent arteriole and drained by an efferent arteriole • Podocytes – epithelial cells covering the glomerular capillaries, forming the filtration membrane Figure 25.7a Nephrons Podocytes – epithelial cells covering the glomerular capillaries, forming the filtration membrane • Foot processes – finger-like extensions of the podocytes that loosely intertwine • Filtration slit – small spaces between the foot processes through which plasma leaks into the capsular space, becoming filtrate Figure 25.7a Nephrons Filtration membrane – the wall through which plasma must cross in order to become filtrate and enter the bowman’s capsule. Consists of the fenestrated endothelium of the glomerular capillaries, the podocytes, and the basement membrane that holds them together Figure 25.7b, c Juxtaglomerular Apparatus JG apparatus – group of receptor cells that regulate the nephrons’ rate of filtration • Granular cells (JG cells) – stretch receptors in the wall of the afferent arteriole. Increased stretch causes vasoconstriction, and decreased stretch causes vasodilation Figure 25.6 Juxtaglomerular Apparatus JG apparatus • Macula densa cells – chemoreceptors for sodium in the wall of the renal tubule. High sodium levels triggers vasoconstriction of the afferent arteriole, and low sodium levels triggers vasodilation. Figure 25.6 Urine Formation Urine is formed in 3 steps: 1. Glomerular filtration – plasma and solutes (valuable and waste) leak from the glomerulus into the bowman’s capsule, forming filtrate 2. Tubular reabsorption – valuable solutes are transported from the filtrate back to the plasma of the peritubular capillaries 3. Tubular secretion – additional wastes are added to the filtrate from the plasma of the peritubular capillaries. The filtrate is now changed to urine Figure 25.8 Glomerular Filtration • Glomerular capillaries are highly porous, leak bout 20% of their plasma • Higher pressure than other capillary beds (55 mmHg) • Net filtration pressure – balance of hydrostatic and osmotic pressures in the glomerulus, forces plasma out to form filtrate • Glomerular filtration rate (GFR) – volume of filtrate formed each minute, normally 125 mL/min Figure 25.9 Regulating Glomerular Filtration Rate Intrinsic Regulation: • Myogenic control – any rise in pressure stretches the afferent arteriole, and JG cells trigger vasoconstriction. A lowered pressure triggers vasodilation • Tubuloglomerular control – a decrease in GFR causes a decrease in filtrate NaCl levels. Macula densa cells then trigger vasodilation. Vasoconstriction is performed when GFR is high and NaCl levels are increased. Figure 25.10 Regulating Glomerular Filtration Rate Extrinsic Regulation: • Renin - Angiotensin mechanism – decreased blood pressure causes JG cells to secrete Renin, causing Angiotensin II production. Causes vasoconstriction and water retention to elevate pressure • Neural control decreased blood pressure causes sympathetic nervous system activity to elevate pressure Figure 25.10 Tubular Reabsorption Reabsorption pathways: • Paracellular – movement of materials between the cells of the renal tubule to access the peritubular capillaries • Transcellular - movement of materials through the epithelial cells of the renal tubule to access the peritubular capillaries • A healthy kidney should reabsorb all nutrients, most water and ions, and some urea. The remaining urea an other nitrogenous wastes are not reabsorbed. Figure 25.11 Tubular Reabsorption • Na+ ions are pumped out of the filtrate via active transport by carriers that simultaneously pump amino acids, glucose and other nutrients • Water, negative ions, some urea, and lipid soluble solutes follow this salt into the peritubular capillaries • Transport maximum – the limited activity of a set number of carriers, additional solutes beyond this amount wind up in the urine Figure 25.12 Tubular Reabsorption • PCT – allows majority of reabsorption including all glucose and amino acids, 65% of sodium, 60% of chloride and more • Loop of Henle – descending limb allows water reabsorption, the ascending limb allows sodium and other ion reabsorption • DCT – allows limited water an ion reabsorption, more if specific hormones are present Figure 25.12 Tubular Secretion • Movement of material from the peritubular capillaries into the filtrate, mostly occurring at the PCT • Secretes some of the urea that was reabsorbed earlier, excess K+ ions, creatinine, and certain drugs • Also secretes excess H+ ions to regulate blood pH Figure 25.8 Regulating Urine Concentration Osmolarity – the number of solutes dissolved in one kg of water. • Note how the gradient of osmolarity increases from cortex to medulla Counter current mechanism – interaction between two adjacent tubules whose contents flow in opposite direction • The two limbs of the loop of henle passing through the osmotic gradient helps with reabsorption and allows the regulation of urine concentration Figure 25.13 Regulating Urine Concentration • The descending limb is permeable to water but not solutes. The filtrate therefore loses water and becomes more concentrated as it descends • The ascending limb is permeable to solutes but nor water. The concentrate filtrate now loses salt and becomes more dilute as it enters the collecting duct. Figure 25.14 Regulating Urine Concentration • In the absence of Antidiuretic Hormone (ADH), the dilute filtrate can be drained as dilute urine • In the presence of ADH, the collecting duct becomes permeable to water which leaks out of the filtrate to form concentrated urine. Some urea follows this water, but this maintains the osmotic gradient Diuretics – chemicals that increase urinary output by inhibiting ADH secretion or sodium reabsorption Figure 25.15 Urine Urine Characteristics: • Color – ranges from clear to deep yellow. Yellowness is due to the presence of urochrome, a pigment from the breakdown of bilirubin • pH – urine is normally slightly acidic, pH near 6, but diet can shift this toward more acidic or alkaline Urine Composition : • 95% water • 5% solutes • Urea – from the breakdown of amino acids • Uric acid – from the breakdown of nucleic acids • Creatinine – from the breakdown of creatine phosphate • Ions – sodium, potassium, bicarbonate, calcium, H+ Figure 25.16 Ureters Ureter – tube to transport urine from the kidneys to the urinary bladder • Lined with a transitional epithelium to allow stretch • Smooth muscle layer moves urine via peristalsis Figure 25.17 Urinary Bladder Urinary bladder – muscular organ that stores urine • Lined with a transitional epithelium to allow stretch • Trigone – triangular region outlined by the openings to the 2 ureters and the 1 urethra • Detrusor muscle – muscle in the bladder wall that contracts during emptying Figure 25.18b Urethra Urethra – tube that drains urine from the bladder and transports it out of the body. Much longer in males because it courses through the penis Internal urethral sphincter – smooth muscle structure surrounding the urethra at the base of the bladder External urethral sphincter – skeletal muscle structure surrounding the urethra in the urigenital diaphragm Figure 25.18a Micturition Reflex Micturition (voiding) – the act of emptying the bladder Micturition reflex: 1. When about 200 mL of urine is collected, stretch of the bladder initiates the reflex causing contractions of the detrusor muscle and relaxation of the internal urethral sphincter 2. Relaxation of the external urethral sphincter can allow micturition, OR contraction of the external urethral sphincter can temporarily inhibit the reflex 3. After an additional 200 mL of urine is collected, the reflex restarts. Figure 25.20a