Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
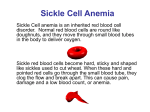
HEMOGLOBINOPATHIES Dr. Swapna V. Goley DEFINITION: Inherited abnormalities of hemoglobin synthesis characterised by structurally abnormal hemoglobin variants. SICKLE CELL ANEMIA • Prototype of hereditary hemoglobinopathies. It occurs due to production of a physiochemically abnormal hemoglobin. It offers a protection against malaria for unknown reasons. • Nearly 20 million people affected in India. • It is inherited as an autosomal recessive trait. • Presents as sickle cell trait (heterozygous) and sickle cell disease(homozygous). • Normal hemoglobin 2 alpha and 2 beta chains form a 4 chain tetramer • HbS: Valine substituted for glutamic acid in both beta chains (HbSS). This occurs due to single point mutation at sixth position of beta globin chain which has thymine instead of adenine. PATHOGENESIS •Due to the change in the amino acid sequence,there is an alteration in charge at the site. •This allows for aggregation & polymerisation of HbS molecules.(formation of tactoids) •Acidosis,Hb concentration,presence of other types of Hb affect polymerisation. •It is a relatively reversible phenomenon but with repeated cycles it becomes irreversible. PATHOGENESIS Arterial pO2 oxyHbS(soluble) Stiff,viscous sickle cell Capillary venule occlusion Microinfarction Ischemic tissue pain Ischemic organic malfn. Venous pO2 deoxyHbS polymerised) Membrane changes Ca2+ influx,K+leakage Shortened red cell survival Anemia, jaundice CLINICAL COURSE • Disease is not evident in newborns. • 2-4 months : Symptoms of Hemolytic Anemia start developing like anemia, jaundice. This is parallel to replacement of HbF by HbS. • 5-6 months : Symptoms arising due to infarction and ischemia start developing. • By the age of 5 yrs almost 95% are functionally asplenic. INFARCTION • Slow, tortuous circulation leads to repeated infarctions. • Effects of the HbS polymerisation, infarction and ischemia are seen in most of the body organs : • Bones • Spleen • Kidney • Lungs • Liver • Brain DACTYLITIS (HAND-FOOT SYNDROME) • First overt manifestation • Painful, usually symmetric swelling with erythema of dorsa of hands & feet. • Sudden in onset and lasts for 1-2 weeks. • Needs medical attention. • Radiographic changes appear 2-3 weeks after appearance of symptoms. SPLENIC INVOLVEMENT •Marked congestion of the red pulp due to trapping of sickled red cells in splenic cords. •The spleen is palpable in most of the children by the age of 9 months.(increased almost up to 500gms.) • Continued scarring causes progressive shrinkage of the spleen. Finally leading to autosplenectomy • Hence they are more prone to infection • Penicillin prophylaxis is begun at 3 months. ACUTE CHEST SYNDROME •Presents with tacypnea,fever,cough,chest pain,arterial O2 desaturation. •Can mimic pneumonia,pulmonary embolism. •Thought to reflect in situ sickling within the lung causing temporary and permanent dysfunction. PNEUMONIA Frequently seen in children with SCA, has high severity because of the relative immunodeficiency. The commonest organism is pneumococcus. GALL STONES Frequent complication of hemolytic anemias OTHER FEATURES •Abdominal crises: severe abdominal pain & signs of peritoneal irritation. •Aplastic crises: infection in adult sicklers with parvovirus B19 results in severe red cell aplasia. •Liver cells may undergo sequestration with severe pain due to capsular stretching. •Aseptic necrosis of head of femur,humerus. •Chronic osteomyelitis: Salmonella sp. most frequently seen organism. •Priapism: due to pooling of blood in corpora cavernosa. •Chronic leg ulcers: seen in adult sicklers. Non healing ulcers usually present on the medial aspect of leg. •Eyes: retinal infarcts, preretinal hemorrhage. •Kidney:limited capacity of H+ excretion,hematuria,hypoastheniuria. •CNS:strokes, focal deficits may occur. DIAGNOSIS • Evidence of red cell destruction: • peripheral blood smear • plasma haptoglobin,hemopexin • Evidence of red cell generation: • reticulocytosis, extramedullary hematopoeisis • Laboratory diagnosis • Blood picture Marrow expansion Hair on end appearance LAB DIAGNOSIS • SICKLE TEST:Red cells with HbS take a sickle shape when mixed with a freshly prepared solution of the reducing agent sodium metabisulphite.(2%) Giving an appearance of turbidity. • SOLUBILITY TEST:Hb added to solution of sodium dithionite(reducing agent) in phosphate buffer.Turbidity shows presence of HbS. • Hb ELECTROPHORESIS Hb ELECTROPHORESIS BLOOD PICTURE • Hb : 6-9gm%, may be lower • Anemia: normocytic,normochromic • MCV,MCH: Normal • Stained film:Moderate anisopoikilocytosis,sickle cells,oval cells,occ target cells,Howell-Jolly bodies • Reticulocytosis (10-20%) MANAGEMENT •Vaso-occlusive crises managed by aggressive rehydration, oxygen therapy, adequate analgesia and antibiotics. •Prophylactic antibiotics: Penicillin prophylaxis to protect against infections which are lethal in presence of asplenia. •Vaccination against pneumococcus, hepatitis B and haemophilus. • Transfusion to suppress HbS production and maintain HbS levels below 30%. • Fetal Hb induction with hydroxyurea (hydroxycarbamide) replaces some HbSS with HbF. As high level of HbF inhibits polymerization • Bone marrow or stem cell transplant appears to be potentially curative. • PROPHYLAXIS Factors that promote sickling should be avoided that is hypoxia, dehydration, acidosis etc. OTHER HEMOGLOBINOPATHIES •Hemoglobin H. Hemoglobin H is a tetramer composed of four beta globin chains. Hemoglobin H occurs only with extreme limitation of alpha chain availability. Hemoglobin H forms in people with three-gene alpha thalassemia •Hemoglobin Barts. Hemoglobin Barts develops in fetuses with four-gene deletion alpha thalassemia. Due to this deletion no alpha chain is produced. The gamma chains produced during fetal development combine to form gamma chain tetramers. These molecules transport oxygen poorly. Most individuals with four-gene deletion thalassemia and consequent hemoglobin Barts die in utero (hydrops fetalis). •Hemoglobin C. Hemoglobin C results from a mutation in the beta globin gene and is the predominant hemoglobin found in people with hemoglobin C disease. (a2bC2).It has Lysine for glutamic acid at 6th position in beta chain. Hemoglobin C disease is relatively benign, producing a mild hemolytic anemia and splenomegaly. Hemoglobin C trait is benign. •Hemoglobin E. This variant results from a mutation in the hemoglobin beta chain. People with hemoglobin E disease have a mild hemolytic anemia and mild splenomegaly. Hemoglobin E trait is benign. •Hemoglobin D: It has the glutamic acid at the 121st position on the beta chain instead of glutamine. It is relatively benign, producing a mild hemolytic anemia and splenomegaly. •Other examples: Hb-Koln, Hb-Zurich, HbSydney, HbO-Arab etc. THANK YOU