Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
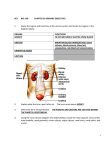
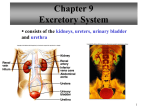
Functional Human Physiology for Exercise and Sport Sciences The Urinary System: Renal Function Jennifer L. Doherty, MS, ATC Department of Health, Physical Education, and Recreation Florida International University Functions of the Urinary System The kidneys remove metabolic wastes from the blood and excrete them to the outside of the body in the form of urine The careful regulation of renal activity keeps blood composition and body fluids within normal limits The kidneys also… Maintain electrolyte and acid-base balance in body fluids Regulate plasma pH by regulating the concentration of bicarbonate ions and hydrogen ions Regulate the volume, composition, and pH of blood Regulate plasma osmolarity and chemical composition Assist in the regulation of BP Regulate plasma volume and produces renin to regulate BP Assist in the regulation of RBC production Regulate RBC production by producing erythropoietin to stimulate RBC formation in bone marrow Assist in the regulation of Ca++ absorption Metabolize vitamin D to its active form, which affects the rate of Ca++ absorption from the small intestines Anatomy of the Urinary System Structures of the urinary system Kidneys (2) Form urine Renal arteries and veins Ureters (2) Tubes for transport of urine from the kidneys to the bladder Urinary bladder (1) Storage reservoir for urine Urethra (1) Transport tube for urine to the outside of the body Microscopic Anatomy of the Kidneys The nephron is the structural and functional unit of the kidney. Each kidney contains about one million nephrons Nephrons consist of: The renal corpuscle Proximal convoluted tubule Loop of Henle Distal convoluted tubule Collecting duct Empties urine into the minor calyx The Nephron: Renal Corpuscle The renal corpuscle consists of… Glomerulus Glomerular Capsule The Nephron: Renal Corpuscle The Glomerulus is the filtering unit of the nephron Tangled cluster of capillary beds lying between the afferent and efferent arterioles Contained within the glomerular capsule The Nephron: Renal Corpuscle The Glomerular Capsule (Bowman’s capsule) is a thin walled, cup-shaped structure surrounding the glomerulus It leads to the renal tubule It receives fluid that filters through the glomerulus Basic Renal Exchange Processes Nephrons function to… Remove wastes from the blood Regulate water and electrolyte concentrations Urine is the end product of these functions The following 3 exchange processes occur within the nephrons Glomerular Filtration Reabsorption Secretion Glomerular Filtration This is the beginning of urine formation Glomerular capillaries are extremely permeable compared to systemic capillaries Hydrostatic and Osmotic Pressure Gradients Greater inside glomerular capillaries Forces water and dissolved solutes to leave the blood plasma in the glomerular capillaries and cross the glomerular membrane into the glomerular (Bowman’s) capsule Filtrate Water and dissolved solutes in the glomerulus Glomerular Filtration The glomerular membrane Separates glomerular capillary blood from the glomerular capsule space Contains many small pores that allow almost all materials to pass through the membrane Exceptions: formed elements Glomerular Filtration Glomerular filtrate Contains water and dissolved solutes that have been filtered from the blood plasma in the glomerular capillaries and collected by the glomerular capsule Similar to tissue fluid containing water, glucose, amino acids, urea, uric acid, creatine, creatinine, sodium, chloride, potassium, calcium, bicarbonate, phosphate, and sulfate ions Will be processed by the renal tubules to form urine Glomerular Filtration A nonselective, passive process Water and dissolved solutes from the blood plasma in glomerular capillaries are forced through the glomerular membrane by hydrostatic and osmotic pressure gradients Water and dissolved solutes travel down their pressure gradients Glomerular Filtration Glomerular Filtration Pressure (Net Filtration Pressure) The net force acting to move materials out of the glomerulus (glomerular capillaries) and into the glomerular capsule Filtration pressure is much higher in the glomerular capillaries compared to systemic capillaries because of: The high permeability of the glomerular membrane It is more permeable than systemic capillary membranes High glomerular blood pressure (60 mmHg) It is higher compared to systemic capillary blood pressure (41 mmHg) Glomerular Filtration Starling Forces Represent the overall effect of all the forces operating at the glomerular membrane Glomerular Filtration: Starling Forces Forces favoring filtration are the forces driving fluid and solutes out of the glomerular capillaries Glomerular capillary hydrostatic pressure PGC = 60 mmHg The primary force pushing water and solutes out of the glomerular capillaries Osmotic pressure in the glomerular (Bowman’s) capsule πBC = 0 mmHg Negligible since few plasma proteins are normally present in the glomerular capsule Glomerular Filtration: Starling Forces Forces opposing filtration are the forces driving fluid and solutes back into the glomerular capillaries Glomerular (Bowman’s) capsule hydrostatic pressure PBC = 15 mmHg Exerted by the fluids within the glomerular capsule Osmotic pressure in the glomerular capillaries πGC = 29 mmHg Due to the plasma proteins in glomerular blood Glomerular Filtration Pressure Glomerular Filtration Pressure Equation Filtration pressure = (forces favoring filtration) - (forces opposing filtration) Forces favoring filtration (glomerular capillary hydrostatic pressure + capsular osmotic pressure) Forces opposing filtratrion (capsular hydrostatic pressure + glomerular capillary osmotic pressure) Values (60 mmHg + 0 mmHg) - (15 mmHg + 29 mmHg) = 16 mmHg Glomerular Filtration Rate (GFR) GFR = the amount of filtrate produced in the kidneys per minute Normal values: 125 ml/min (180 L/day) GFR varies with the filtration pressure All the factors that affect glomerular filtration pressure will affect the GFR Glomerular capillary osmotic pressure Glomerular capillary hydrostatic pressure Glomerular capsule osmotic pressure Glomerular capsule hydrostatic pressure Glomerular Filtration Rate (GFR) Glomerular capillary hydrostatic pressure ↑ glomerular capillary hydrostatic pressure = ↑ GFR Glomerular capsule osmotic pressure ↑ glomerular capsule osmotic pressure = ↑ GFR Glomerular capillary osmotic pressure ↑ glomerular capillary osmotic pressure = ↓ GFR Glomerular capsule hydrostatic pressure ↑ glomerular capsule hydrostatic pressure = ↓ GFR Glomerular Filtration Rate (GFR) GFR varies with the rate of blood flow through the glomerular capillaries To maintain a high GFR, blood must flow quickly through glomerular capillaries Vasocontriction or vasodilation in the glomerular arterioles elicit changes in the glomerular filtration pressure Changes in the glomerular filtration pressure effect GFR Glomerular Filtration Rate (GFR) Vasoconstriction of the afferent arterioles or vasodilation of the efferent arterioles ↓ glomerular capillary hydrostatic pressure ↓ GFR Vasodilation of the afferent arterioles or vasoconstriction of the efferent arterioles ↑ glomerular capillary hydrostatic pressure ↑ GFR Regulation of GFR GFR remains relatively constant May be ↑ or ↓ according to the body’s need Mechanisms of regulation: Intrinsic control (Autoregulation) Myogenic regulation Tubuloglomerular feedback Extrinsic control Renal blood flow Exercise Regulation of GFR: Intrinsic Control The ability of the kidney to maintain a constant blood flow when arterial BP is changing The ability of the kidneys to maintain a relatively constant GFR when mean arterial pressure is changing This mechanism is effective over the "normal" range of arterial BP 80 - 120 mmHg Regulation of GFR: Intrinsic Control Myogenic Regulation Related to the inherent property of smooth muscle to contract when stretched ↑ mean arterial pressure = ↑ stretch of smooth muscle in the afferent arteriole walls stimulating vasoconstriction Vasoconstriction of the arterioles causes a decrease in glomerular capillary hydrostatic pressure This protects the delicate glomerular capillaries from high mean arterial pressures Myogenic regulation is especially effective in the afferent arteriole Regulation of GFR: Intrinsic Control Tubuloglomerular Feedback Negative feedback system GFR is regulated by changes in flow of tubular fluid past the macula densa Specialized cluster of epithelial cells in the distal convoluted tubule near the afferent and efferent arterioles Changes in Na+ and Cl- concentration in the filtrate are detected by osmoreceptors in the macula densa Tubuloglomerular Feedback Macula Densa Cells Respond to changes in the Na+Cl- concentration in the filtrate in the distal convoluted tubule ↓ Na+Cl- concentration = afferent arteriole vasodilation Vasodilation of the afferent arteriole results in: ↑ blood flow to the glomerular capillaries ↑ glomerular filtration pressure ↑ GFR The opposite is also true Tubuloglomerular Feedback Juxtaglomerular Cells Contain mechanoreceptors that stimulate the juxtaglomerular cells to release renin in response to changes in mean arterial pressure Renin is an enzyme that catalyzes a cascade of reactions in the bloodstream Renin converts angiotensinogen → angiotensin I Angiotensin converting enzyme (ACE) converts angiotensin I → angiotensin II Angiotensin II is the most powerful vasoconstrictor in the body Increases mean arterial blood pressure Tubuloglomerular Feedback Activation of the juxtaglomerular cells to release renin occurs when there is a decrease in mean arterial pressure Usually when mean arterial pressure is less than 80 mmHg Direct activation of juxtaglomerular cells Achieved via the mechanoreceptors sending impulse through the sympathetic nervous system Indirect activation of juxtaglomerular cells Achieved via the macula densa cells which detect changes in Na+Cl- concentrations in the filtrate Macula densa cells cause vasoconstriction or vasodilation, which alters mean arterial pressure as detected by the juxtaglomerular cells Regulation of GFR: Extrinsic Control Renal Blood Flow The sympathetic nervous system is able to override autoregulation of the kidneys ↑ sympathetic input = ↓ GFR Sympathetic input causes vasoconstriction of both afferent and efferent arterioles, thereby decreasing GFR Regulation of GFR: Extrinsic Control Exercise Exercise results in increased sympathetic nerve impulses Sympathetic nerve impulses stimulate the adrenal medulla to release epinephrine, which stimulates… Release of renin = ↑ mean arterial pressure Vasoconstriction of the afferent arteriole = ↓ GFR Reabsorption The process of reclaiming fluid and solutes from the filtrate in the renal tubules Reabsorption occurs in the peritubular capillaries Solutes and water move from the lumen of the renal tubules back into the plasma If reabsorption did not occur, a person would lose 1L of fluid in the urine in 8 min Solute Reabsorption Substances are selectively reabsorbed from the filtrate Peritubular capillaries are specially adapted for the process of reabsorption Under very low BP Walls are very permeable Reabsorption occurs throughout the renal tubule; however, most reabsorption occurs in the proximal convoluted tubule Solute Reabsorption: Proximal Convoluted Tubule Most reabsorption occurs in the proximal convoluted tubule Proximal convoluted tubule contains epithelial cells with microvilli Microvilli increase the surface area within the renal tubules Solute Reabsorption: Proximal Convoluted Tubule Solutes are moved from the tubule lumen, across the apical membrane, into the epithelial cells lining the tubule walls Solute Reabsorption: Proximal Convoluted Tubule Solutes then move out of the epithelial cells lining the tubule walls, across the basolateral membrane, into the peritubular space Solute Reabsorption: Proximal Convoluted Tubule From the peritubular space, solutes easily diffuse into the peritubular capillaries Regional Specialization of the Renal Tubules: Proximal Tubule Na+ ions are actively reabsorbed by active transport Requires ATP Reabsorption of Na+ establishes an electrical gradient for reabsorption of negatively charged ions As positively charged Na+ ions are transported out of the filtrate, negatively charged ions accompany them via passive diffusion 1) Cl2) Bicarbonate (HCO3-) Reabsorption of Na+ also establishes an osmotic gradient for the reabsorption of water Water is passively reabsorbed by osmosis and returned to the systemic circulation by the peritubular capillaries Regional Specialization of the Renal Tubules : Proximal Tubule The mechanisms of reabsorption in the proximal tubule are so efficient that 70% of water and Na+ filtered is reabsorbed before the tubular fluid reaches the loop of Henle Water and Na+ reabsorption are regulated by several hormones At the end of the proximal convoluted tubule, the filtrate and the blood in the peritubular capillaries are isotonic (electrically neutral) Regional Specialization of the Renal Tubules : Distal Tubule Major function is regulation of Na+ and Clconcentration of the filtrate The primary site of aldosterone activity Aldosterone increases Na+ reabsorption and K+ secretion In the presence of aldosterone, the distal convoluted tubule will actively reabsorb Na+ and Cl When Na+ is reabsorbed, water reabsorption also occurs Results in increased blood volume and BP Transport Maximum There are different modes of transport that may be used to reabsorb substances in particular segments of the renal tubule Solutes are transported from filtrate to plasma across the tubular epithelium by carrier proteins or pumps Carrier proteins may become “saturated” When solute concentration is high enough, all carrier proteins and pumps are occupied When all carrier proteins and pumps are occupied, the system is operating at Transport Maximum Transport Maximum Glucose Reabsorbed via active transport Renal tubule epithelial cells contain special protein transporters that remove glucose from the tubular filtrate When the plasma and filtrate concentration of glucose are high enough to saturate all carrier sites, the excess glucose will end up in the urine This is the renal plasma threshold for glucose Transport Maximum When the concentration of a substance in the filtrate exceeds its renal plasma threshold, the excess is excreted in the urine Example: Diabetes Mellitus (Type I insulin dependent) Excess glucose in the urine provides an osmotic gradient Glucose in the filtrate will draw water into the renal tubule by osmosis and increases the urine volume This is called osmotic diuresis In chronic conditions osmotic diuresis can lead to kidney damage Reabsorption: Summary Some substances are not reabsorbed at all Found in the urine Some substances are reabsorbed incompletely Found in the urine Some substances lack carriers, are not lipid soluble, or are too large to pass through the membrane pores of the tubular cells Found in the urine The concentration of substances that remain in the filtrate increases as water is reabsorbed Secretion The movement of solutes from the blood in the peritubular capillaries into the lumen of the renal tubules Secretion occurs primarily in the proximal and distal convoluted tubules Substances secreted by the kidneys into urine are: H+ K+ Urea Creatinine Ammonia (NH3+) Histamine Secretion Functions of the secretion process: Helps maintain normal blood concentrations of certain electrolytes Eliminates excess K+ Helps maintain normal pH of body fluids Eliminates undesirable substances that have been reabsorbed Urea Uric acid Secretion Active Secretion Some substances are secreted actively in the proximal and distal convoluted tubules These substances include various organic compounds and H+ ions Acidosis (decreased pH) is controlled by the renal tubule cells Actively secrete H+ ions Actively retain bicarbonate and K+ ions Secretion Passive Secretion K+ ions are secreted passively in the Distal convoluted tubule Collecting duct K+ ions are attracted to the negative charge that develops in the lumen of the renal tubule Excretion The elimination of solute and water from the body in the form of urine Micturition = the process of urination Substances that enter the lumen of the renal tubules are excreted unless they are reabsorbed Substances may enter the renal tubules by either filtration or secretion Excretion Excretion Rate The rate in which a substance is excreted depends on… The quantity of a certain solute that is filtered at the glomerulus per unit time (filtered load) The rate at which a solute is secreted The rate at which a solute is reabsorbed Regulation of Urine Concentration and Volume While the function of the proximal convoluted tubule is to reabsorb most of the water and Na+ out of the tubular filtrate The role of the Loop of Henle is to adjust the concentration and volume of urine The juxtamedullary nephrons are particularly suited to adjust the concentration and volume of urine because their nephron loops descend deep into the renal medulla By the end of the proximal convoluted tubule, the filtrate volume has decreased by 80 - 85% and the remaining fluid is isotonic The Loop of Henle Descending limb Descends toward the medulla of the kidney The fluid surrounding the nephron loop is called the medullary interstitial fluid As the nephron loop decends into the medulla of the kidney, the medullary interstitial fluid becomes more concentrated The Loop of Henle The osmolarity of the medullary interstitial fluid increases from 200 mOsm in the renal cortex to about 1200 mOsm in the deepest parts of the renal medulla The increase in osmolarity is due to Na+ ions that are concentrated in the renal medulla by the countercurrent multiplier Countercurrent Multiplier Involves interactions between the flow of filtrate through the Loop of Henle and the flow of blood through the adjacent blood vessels, the vasa recta Countercurrent refers to the opposite direction of flow in the Loop of Henle and the vasa recta Countercurrent Multiplier The concentration of filtrate leaving the proximal convoluted tubule and entering the nephron loop is isotonic Filtrate contains concentrations equal to the blood plasma and the interstitial fluid of the renal cortex Urine that is excreted must be more concentrated than blood plasma The kidney achieves this goal through the countercurrent multiplier effect The Countercurrent Multiplier Effect Refers to filtrate flowing in opposite directions in the descending and ascending limbs of the Loop of Henle Because of this countercurrent flow, small differences in the concentration of the filtrate in the descending and ascending limbs results in a large medullary interstitial fluid concentration gradient The medullary interstitial fluid concentration gradient is established by the following mechanisms: Permeability of the descending loop Permeability of the ascending loop Permeability of the vasa recta The Countercurrent Multiplier Effect Descending limb of the nephron loop Very permeable to water A relatively high Na+ concentration remains in the filtrate as it reaches the ascending limb Ascending limb of the nephron loop Selectively permeable Na+ is removed from the filtrate but water is not Na+ becomes concentrated in the medullary interstitial fluid The vasa recta Highly permeable to Na+ and Cl Responsible for maintaining Na+ and Cl- concentration in the renal medulla The Countercurrent Multiplier Effect Increased concentration of the medullary interstitial fluid increases the osmotic pressure in the renal medulla More Na+ remains in the medullary interstitial fluid As a result of the countercurrent multiplier effect, small differences in the osmolarity of the filtrate in the ascending and descending nephron loops creates a large medullary concentration gradient The medullary concentration gradient serves as the driving force for urine concentration The Collecting Duct By now, the filtrate is called urine The major function of the collecting duct is regulation of water reabsorption Therefore, it is the primary site of antidiuretic hormone (ADH) activity ADH from the posterior pituitary gland increases the permeability of the… The distal convoluted tubule The collecting duct The Collecting Duct No ADH present The epithelial cells of the collecting duct are relatively impermeable to water Produces dilute urine ADH present The pores in the collecting duct enlarge and increase the permeability to water Results in greater reabsorption of water 1) Reduced urine volume 2) Urine is very concentrated Micturition Voiding or eliminating urine Expulsion of urine from the bladder Involves contraction of the detrusor muscle and relaxation of the external urethral sphincter Distension of the bladder stimulates stretch receptors in the wall of the bladder The stretch receptors stimulate the micturition reflex center located in the sacral region of the spinal cord Micturition Miturition Reflex The micturition reflex center sends parasympathetic motor impulses to the detrusor muscle Parasympathetic impulses to the detrusor muscle stimulates rhythmic contraction and relaxation of the internal urethral sphincter As the bladder fills, its internal pressure increases and opens the internal urethral sphincter A second reflex relaxes the external urethral sphincter Contraction of the external urethral sphincter may be voluntarily controlled Micturition The desire to urinate is stimulated by distention of the bladder Occurs when the bladder fills with ~150 ml of urine Urine volume of ~300 ml or more leads to sensations of uncomfortable fullness At maximum capacity, the bladder may hold ~500 – 600 ml (1 pint) of urine Following urination, less than ~10 ml of urine usually remain in the bladder Micturition Nerve centers in the brain stem and cerebral cortex aid in the control of urination When the need to urinate is sensed, the micturition impulse can be temporarily inhibited through cerebral cortex and midbrain control Voluntarily relaxation of the external sphincter allows urination to occur Urine Composition Urine is ~ 95 % water Also contains urea, uric acid, and creatinine Urine may contain trace amounts of… Amino acids Electrolytes Urine is usually acidic with a pH of ~6 Urine is more acidic than blood plasma and intracellular fluid Urine volume is ~0.6 - 2.5 L/day The glomerular capillaries filter about 180 L/day