Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
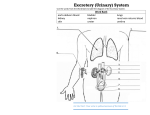
Anatomy and Physiology of the Kidney: A micro-engineering marvel that maintains osmotic homeostasis in our body Larry M. Frolich, Ph.D. Yavapai College, Dept. of Biology Baseline physiology understanding is often common sense: What do you already know about the kidney and what it does? Kidney Brainstorm Take 30 seconds to describe what the kidney does Adjective/phrase 1: Adjective/phrase 2: Adjective/phrase 3: The Challenge: Appreciate the kidney’s elegant fluid flow engineering solution to minimizing fluid loss while maintaining osmotic balance and secreting metabolic waste products To get there, we need to know: Where kidney is located, flow of urine out of body Internal organization of kidney Urine production in kidney—a 3-step process 1. 2. 3. Filtration Reabsorption and Secretion Concentration Diabetes and Kangaroo Rats—do you really understand the kidney? Where are kidneys? Paired, midabdomen Retroperitoneal “kidney punch” “dolor de los riñones” Urine constantly flows to bladder through urethra Urine collects in bladder and passes through urethra at urination Inside the kidney One lobe of kidney is medullary pyramid plus cortex around it Cortex has concentration of glomeruli where filtration happens Medulla or core of pyramid appears striated due to oriented collecting ducts that unite into minor calyx at apex of pyramid Minor calices are open spaces where urine collects at apex of pyramid Minor calices empty into larger major calices which merge to form renal pelvis Urine passes from renal pelvis into ureter Ureter--from kidney to bladder LAYERS OF URETER External connective tissue-adventitia Middle muscular layer-muscularis Smooth Muscle Inner Longitudinal Outer Circular External longitudinal (on distal third) Peristaltic action moves urine to bladder (and stones!!) Inner lining of transitional (stretchy) epithelium--Mucosa Bladder Muscular (what kind?) sac that fills with urine from ureters Anterior against pubis in pelvis Filled with urine expands into abdomen Blood supply from internal iliac arteries Innervation is autonomic from hypogastric plexus Layers of bladder wall Outer connective tissue-adventitia Middle muscular layer (“detrusal” or expulsor)-inner and outer longitudinal fibers around middle circular fibers Inner transitional (stretchy) epithelium Bladder can expand 15 times its empty volume to hold 500 ml of urine Trigone is triangle between ureters/urethra-persistent sight of infection Urethra Drains urine from bladder to outside Female = short tube Males = long tube Prostatic, Membranous, Spongy (penile) portions Also carries sperm Internal Urethral Sphincter Between bladder + urethra Thickening of detrusor (smooth muscle) External Urethral Sphincter Within urogenital diaphragm Skeletal muscle = voluntary control urination External Urethral Orifice Males = end of penile urethra Females = anterior to vaginal opening, posterior to clitoris Micturition = Urination Emptying bladder Stretch receptors in bladder respond when bladder full Parasympathetic signals detrusor muscle to contract and internal urinary sphincter to open (also inhibits sympathetic pathways that would prevent urination) Other brain receptors can inhibit urination by relaxing detrusor, and keep external urinary sphincter closed Voluntary contraction of abdominal wall muscles increases abdominal pressure Voluntary relaxation of external urethral sphincter Ascent of the kidney in development Kidneys from intermediate mesoderm Pronephric kidney in fetus shows segmental body plan Fish with dorsal renal tissue lateral to vertebral column for most of length In human, metanephric kidney migrates from inferior to superior Variation in kidney shape not uncommon (horseshoe kidney Ureter also from intermediate mesoderm Nephron: the functional unit of the kidney (understand how one nephron works and you understand how the kidney works) One million nephrons per kidney (140 miles of tubing within each kidney!) Always oriented with glomerulus towards cortex, collecting duct heading towards calyx at apex of pyramid in center of kidney How does the kidney remove waste products from the blood and maintain osmotic balance in the body? Friedrich Gustav Jakob Henle (1809-1885) (THE STORY OF BOWMAN AND HENLE) Sir William Bowman (1816-1892) Filtration: Bowman’s Capsule 2. Reabsorption and Secretion: Proximal Convoluted Tubules 3. Concentration of Urine: Collecting Duct—Loop of Henle establishes concentration gradient 1. How does a nephron work? 3 Steps—the quick story: 1. Plasma filters out of blood and into tubules at Bowman’s Capsule 2. In tubules, water and non-waste solutes are reabsorbed back into blood. Wastes from blood are secreted into tubules 3. In collecting duct, water osmoses out and urine is concentrated to final form Collecting duct Kidneys are 0.5% of total body weight but receive over 20% of blood pumped by the heart Another view of the same Step 1. Filtration—Bowman’s Capsule/Glomerulus Constant Glomerular Filtration Rate (GFR)—about 100 mL/min = 150 L/day Special epithelial cells (podocytes) surround capillary Fenestrated endothelial cells of capillaries, and slits between podocytes allow plasma with dissolved solutes to leave blood at rapid rate and filter into capsular space Molecules smaller than 3nm filter through including water, electrolytes, glucose, fatty acids, amino acids, nitrogenous wastes. Proteins and cells are too large. PODOCYTES Step 2. Reabsorption and Secretion—PCT Six percent of resting ATP use, or caloric energy is expended here Water, ions, and glucose are reclaimed from glomerular filtrate back into capillaries that surround tubule by reabsorption Sodium is actively pumped across epithelial cells of tubule (Na-K pump using ATP) Wastes including uric acid are secreted from blood in surrounding capillaries into interior of tubule Step 3. Concentration— Collecting Duct. (Loop of Henle creates concentration gradient) Active transport of NaCl on Ascending Loop of Henle sets up countercurrent exchange Concentration gradient into center of medulla allows concentration of urine in collecting duct Hormonal control of permeability of collecting duct membrane determines ultimate concentration of urine Review of nephron function Diabetes and the PCT RESORPTION: DIABETES AND THE PCT Constant thirst and bed-wetting are symptoms of diabetes. Why? High sugar levels in blood leads to high sugar levels in filtrate at glomerulus This sugar-rich filtrate cannot be fully reabsorbed across proximal convoluted tubule resulting in higher volume of fluid, with dissolved sugar left in tubule. This leads a need for more frequent urination (or bed-wetting in children) and frequent thirst to replace lost fluid Early 20th century physicians diagnosed diabetes by tasting the patient’s urine! Kangaroo Rats and the Loop of Henle CONCENTRATION: KANGAROO RATS AND THE LOOP OF HENLE Kangaroo Rats live in extremely arid desert environments They need no water besides what is in the seeds they eat They secrete a powerfully concentrated nearly solid urine Their secret is an extremely long Loop of Henle whose countercurrent exchange produces a concentration of sodium almost four times higher than humans in the interior of their kidney See graphic in next slide NEPHRON OF A KANGAROO RAT