Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
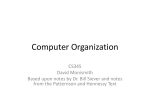
Register-based research in the Nordic countries Mika Gissler Nordic School of Public Health, Gothenburg, Sweden & THL National Institute for Health and Welfare, Helsinki, Finland Why good possibilities to register-based studies? • Traditions: population statistics have been collected more than 250 years and health statistics more than 150 years in the Nordic countries. • First real registers were started in the 1940-1950s, when improved computers were available: health care personnel, cancer register. • Personal identification numbers since 1960s. • Several data quality studies have shown the high quality of routinely collected registers. • Data protection allows research use of register data. Important registers in the Nordic countries • • • • • • • • • Cancer register Registers on infectious diseases Hospital discharge registers Cause-of-death registers Birth and malformation registers Register-based Census Health care quality registers Prescription registers Hospital outpatient registers 1940s 1950s 1960s 1960s 1960s 1990s 1990s 1990s 1990s Unique registers and data in the Nordic countries • IVF (in vitro fertilization) register, Denmark • Register on induced abortions and sterilisations, Finland • Register on visual impairments, Finland • Register on breast and cervical cancer screening, Finland • Multiple generation register, Sweden • Multiple generation studies in the Norwegian Medical Birth Register • Biobanks in all Nordic countries + possibilities to link them to other registers. Important registers for studies in psychiatry and mental health • • • • • • Hospital discharge registers Cause-of-death registers Pension Registers Register-based Census Prescription registers Hospital outpatient registers 1960s 1960s 1960s 1990s 1990s 1990s Examples of register-based studies in psychiatry and mental health • Register-based studies: – Cross-sectional studies – Trends – Longitudinal studies • Combination of data from different sources: – Medical records – Questionnaires – Biobank material Example 1: Life expectancy among psychiatric patients • Registers: – THL: Hospital Discharge Register 1980-2003 – Finnish Centre of Pension: Pension Register 1980-2003 – Statistics Finland: Cause-of-Death Register 1981-2003 • Data: – The data included 361 898 persons aged 15 years or more – 17 638 persons with dementia and 2 630 with intellectual disability were excluded • Life expectancy at 15 years and for ages 15-64 years were calculated separately by using Wiesler's method. Life expectancy increased 80 70 60 50 40 30 Finland Psychatric patients 20 10 Men Women 2001-03 1996-00 1991-95 1986-90 1981-85 2001-03 1996-00 1991-95 1986-90 1981-85 0 Conclusions • Life expectancy at 15 years has increased among Finnish population with hospital discharge or pension due to mental disorders between 1981 and 2003: – Finland: +3.5 years, psychiatric patients +5.8 years • F30-39: +10 years, F40-49: +8 years, F20-29: +6 years, but • F10-19: -0.6 years • Risk for death – diseases and medical conditions – external causes and poisoning 2-fold 6-fold • Similar results from other Nordic countries. Example 2: Maternal smoking and children’s F-diagnoses • Registers: – THL: Medical Birth Register 1987-1989 – THL: Hospital Discharge Register 1987-2007 – Social Insurance Institute: Reimbursed psychotropic medicine 1994-2007 – Statistics Finland: Cause-of-Death registers 1987-2008 • Data: – Children born in 1987-1989, excluding perinatal deaths, multiples, and children with major congenital anomalies – Final study population: 175 869 children (94.4%) Risk for adverse psychiatric outcomes by maternal smoking 2.50 2.00 1.50 Inpatient care Outpatient care 1.00 Death Psychotropic medication 0.50 0.00 No smoking < 10 cig > 10 cig Crude No smoking < 10 cig > 10 cig Adjusted Adjusted by maternal age, parity, sex, gestational age, birth weight, 5 minute Apgar score and maternal psychiatric diagnosis before birth. Conclusions • Children exposed to maternal smoking has an increased risk for receiving a F-diagnosis in inpatient or outpatient care in childhood and adolescent. • The increased risk can be observed for all diagnosis excluding schizophrenia and anorexia. • Register studies cannot confirm the real effect of smoking. – However, a recent local study in Turku has shown that prenatal smoking exposure is associated with smaller regional brain volumes in preterm infants (Ekblad et al., J Pediatrics 2009). Example 3: Use of psychotropic drugs and pregnancy outcomes • Registers: – The ‘Drug and Pregnancy’ -database 1996-2006, to be annually completed 2007 onwards • Data: – All births in the Medical Birth Register – All induced abortions in the Abortion Register – All congenital anomalies in the Malformation Register • Use of prescribed & reimbursed drugs (Social Insurance Institution) – 3 months before pregnancy – during pregnancy – 3 months after pregnancy The use of psychotropic medicine before the pregnancy starts • The Drug and Pregnancy -database 1996-2006: – Total 622 671 births and 117 229 induced abortions – Excluded: induced abortions due to fetal reasons – Separate analysis: first pregnancies • All drug purchases 3 months before pregnancy were used as a proxy measure of mental health disorders. Conclusions • Measured by the use of psychotropic medicine, women’s pre-existing mental health status is worse for women having an induced abortion than for women giving a birth. – All pregnancies: Adjusted OR 1.94 (95% CI 1.87-2.02) – First pregnancies: Adjusted OR 1.56 (95% CI 1.44-1.68) – Highest risk for women using hypnotics and sedatives, antipsychotics and antidepressants. • This essential confounding factor should not be neglected when investigating the occurrence of pregnancy-related mental health problems. Example 4: Mothers’ and children’s longterm follow-up after substance abuse during pregnancy • Basic data: – 524 women followed-up prenatally at special out-patient clinics and a control group of 1792 women matched for maternal age, parity, time and place of delivery. • Registers: – THL: Medical Birth Register, Hospital Discharge Register, Child Welfare Register – Statistics Finland: Cause-of-Death Register – Social Insurance Institution: Information on prescribed medicine, social benefits, pensions and rehabilitations Mothers’ outcome, % • • • • • • • Death F-diagnosis, inpatient F-diagnosis, outpatient Intoxication care Pensions, any cause Rehabilitation, any cause Special reimbursement – Psychosis • Drug reimbursement N05 • Drug reimbursement N06 Cases Controls 8.0 46.0 47.1 41.3 16.8 9.5 27.0 0.2 3.6 8.3 1.8 2.2 5.6 18.4 *** *** *** *** *** *** *** 10.9 1.4 *** 71.4 68.1 20.9 *** 26.5 *** Children’s outcome, % • • • • • • • • • Death F-diagnosis, inpatient F-diagnosis, outpatient Care benefit for sick child Rehabilitation, any cause Special reimbursement Drug reimbursement N05 Drug reimbursement N06 Child taken into custody Cases Controls 1.4 7.1 8.1 25.0 5.1 12.1 9.1 4.6 46.0 1.0 2.8 2.6 13.9 2.4 11.1 5.6 1.4 2.4 NS *** *** *** *** NS ** *** *** Conclusions • • • Combination of medical records and registers was feasible, even though it was difficult to get all the necessary permissions. Women with substance abuse displayed significant long-term abuse-related morbidity and mortality, rehabilitation, early retirement, and use of prescribed medicine. Also their children had increased morbidity, rehabilitation, and use of prescribed medicine, and almost half of them were taken into custody. Why register research? • Easy to form data: – cross-sectional studies – longitudinal studies (history, follow-up) • • • • • • • Easy to repeat the same study. No limitations for sample size (rare cases --- total population). Population-based studies feasible. No need to contact patients. Follow-up relatively easy. No participation bias nor research bias. No reporting bias. Problems related to register research • The data is unavailable – primary health care, diseases and conditions not requiring a contact to health care system, self-rated health, opinions, experiences,... • Data protection: are such studies possible in general? • Ethically controversial topics: – abortion, miscarriage, infertility, malformations, psychiatric disorders, family studies, contact to relatives of a death patient, genetics… • High data costs: Statistical offices, Central Population Register • Data overload syndrome – Too much data, too little time…? • Fishing: – Easy to find statistically significant results, if the data is large. Finally • Register-based studies seems to be feasible, e.g. for cross-sectional, longitudinal and trend studies • Combination of data from other registers and from other sources, such as medical records, questionnaires and even biobank material is possible. • Data protection questions have not been an issue, at least until now. • The lack of information from primary health care will be solved after the national electronic patient journal system is in use. Promotion of register research • Denmark: National Centre for Register-based Research, Århus Universitet http://www.ncrr.dk/ • Finland: Finnish Information Centre for Register Research http://www.rekisteritutkimus.fi/ • Norway: Special issue on register-based research in Norsk Epidemiologi 14 (1): 2004. • Sweden: Grants for register-based research by the National Board of Welfare and Health (Socialstyrelsen)