Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
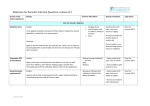
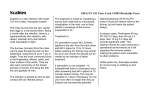
ADL- Cirujales,MD 1. Discuss common arthropods that can infest the human body. 2. Identify cutaneous reactions and systemic manifestations that occur with infestations and bites. 3. Relate the life-cycle of commonly identified arthropods to the clinical presentation and management of the disease. 4. Identify the diagnostic tools or procedure for the different disease condition. 5. Enumerate important health teachings that can be incorporated in the community and clinical setting. ARACHNIDA CHILOPODA Acarina (Scabies) Aranea (Brown Recluse Spider) DIPLOPODA INSECTA Anoplura (Pediculosis) Hemiptera (Bedbugs) Family Sarcoptidae Class Arachnida Obligate human parasite Oval in shape Pearl-like, translucent, white Adult F mite 0.4x0.3mm Eyeless 4 short, stubby legs Cannot fly or jump Worldwide All ages All races Socioeconomic status Epidemic or endemic scabies in institutions “It has been well established that close personal contact is a prime route of transmission.” “…the equally high prevalence in children attests that casual contact or sharing of objects among children and family members is also sufficient to transmit the disease.” Fitzpatrick’s Dermatology in General Medicine 8 th edition “ Mites are also prevalent in the personal environment of normal scabies person.” “In one study, live mites were recovered from dust samples taken from bedroom floors, overstuffed chairs and coaches in every patient’s dwelling.” Fitzpatrick’s Dermatology in General Medicine 8th edition F mite forms burrow Lay 2-3 eggs/day Eggs hatch (4d;10d) Live burrow to mature on the skin surface M and F mite copulate M mite falls off gravid F burrows Hypersensitivity Reaction immediate reaction delayed type 1st infestation sensitization to S.scabiei 4-6 weeks pruritus Reinfestation pruritus within 24H Pruritic papular lesions Intraepidermal burrows Secondary changes -excoriations -LSC -PIH -secondary infection by Staph aureus Dull, red nodules +/- pruritus Scrotum, penis vulva Immunocompromised, debilitated, patients w/ neurologic D/O Crusts, scales, mites Face, scalp Nails- psoriasis-like scaling, distorted Tips of fingers swollen and crusted Severe fissuring and scaling of genitalia & buttocks Rub a black felt-tip marker across the affected area Wipe excess ink with an alcohol pad Burrow would appear darker than the surrounding skin Identification of the burrow: india ink or gentian violet Drop mineral oil over the burrow Scrape off burrow with curette or no. 15 blade Microscope slide Microscopy Microscopic identification of the ff: 1. S. scabiei mites 2. eggs 3. fecal pellets (Scybala) Highest yield in identifying is in typical burrows: 1. finger webs 2. flexor aspect of the wrists 3. penis Located stratum corneum F mite with eggs in the blind end of the burrow Spongiosis (epidermal edema) Eosinophilic infiltrates (dermis) 1. Treat infested individual and close physical contact (including sexual partners) at the same time whether or not symptoms are present. 2. Scabicide + fomite control 3. Second application a week after initial tx. 1. 2. Permethrin 5% cream 1. Lindane 1% lotion or cream 3. 2. 4. 5. Recommended Regimen Crotamiton 10% Sulfur 2-10% in petrolatum Benzyl Benzoate w/ sulfiram Sulfram 25% Ivermectin 0.8% Alternative Regimens Ivermectin -200ug/kg single dose -2 to 3 doses separated by 1 to 2 wks (heavy infestation; immunocompromised state) -Epidemic and endemic scabies -Not approved by US FDA -C/I: infants, young children, pregnant and lactating women 1. Post-scabetic itching 2. Secondary Bacterial Infection 3. Scabietic nodules - IL Triamcinolone 5-10 mg/mlinto each lession is effective - repeat every 2 weeks if necessary All clothing, pillow cases, towels, bedding used during the previous week should be washed in hot water and dried at high heat Nonwashables should be dry-cleaned, ironed, put in clothes dryer w/o washing or stored in a sealed plastic bag in a warm area for 2 weeks Floors, carpets, upholstery (home & car), play areas, furniture should be carefully vacuumed Fumigation not recommended Pets do not need to be tx bec they do not harbor the human scabies mite Loxosceles reclusa Fiddle-back spider Yellow, tan or brown 10-15mm long Leg span 25 mm South Central United States Shy, nocturnal Non-aggressive arachnid Lives in dark areas like woodpiles, under rocks or in dark corners of attics, garages or basements Major cause of necrotic arachnidism in the US Humans come in contact with spider accidentally Bite frequently goes unnoticed 6-8 hours later, local vasospasm (localized, pain, stinging and burning) 12-24H later, systemic symptoms (fever, chills, nausea, vomiting, weakness, joint and muscle pain) Tissue necrosis occur D/T SPHINGOMYELINASE D Cutaneous loxoscelism Systemic loxoscelism Localized hive-like reaction, minimal redness & swelling Cyanotic color followed by expanding necrosis Most severe reaction in fatty areas- thighs, abdomen & buttocks DERMONECROSIS may leave an ulcer that takes months and years to heal Neck-upper airway obstruction Histology depends on the time biopsy was taken Early in the course – (+) neutrophils; (+) “mummified” coagulative necrosis of the epidermis, adnexae & dermis Vasculitis in larger vessels Ecthyma Gangrenosum Necrotizing Vasculitis Necrotizing Fascitis Pyoderma Gangrenosum Polyarteritis Nodosa Supportive care Mild, localized reaction- rest, ice, elevation Necrotic skin – local wound and ulcer care Antibiotics Tetanus toxoid Dapsone 50-100mg/day is helpful in preventing severe necrosis Pediculosis Humanus Capitis (Head Louse) Pediculosis Humanus Humanus (body, clothing louse) Phthirus Pubis (pubis, crab louse) Flattened Wingless 3 pair of legs that terminate in sharp claws used to grasp and hold Obligate human parasite Blood meal q 4-6H 3-12 y/o F>M Rare in AfricanAmerican Direct head to head contact Indirect contact ◦ Can be easily dislodged by air movements, blowdryers, combs and towels ◦ Passively transferred to fabric facilitating new infestation F louse lay 5-10 eggs/day Eggs hatch (10 days) Larvae/nymphs/instars 3 stages of dev’l Full maturation day 14 Nits within 4mm of scalp suggest active infestation Newly-laid or viable eggs are tan to brown Non-viable eggs are clear, white or light in color Presence of adult lice confirms active infestation Incubation of 4-6 wks ◦ Pruritus Carriers ◦ Asymptomatic despite infestation Papular urticaria on the neck Eczema, excoriations, LSC ( occipital scalp) Infection Post occipital lymphadenopathy Small white hair “beads” hair casts, hair lacquer, hair gels, dandruff Scalp pruritus AD, Impetigo, LSC No infestations Delusions of Parasitosis (+) DETECTION OF LICE Louse comb increases chances of finding lice EYE or MICROSCOPY Nits 0.5mm, oval, whitish eggs Nonviable nits Absence of embryo or operculum Louse Insect with 6 legs; 1-2mm length; wingless; translucent, grayish white body that is red when engorged with blood Topically applied Permethrin Malathion Pyrethrin Piperonyl Butoxide Variable ovicidal activity Pt’s compliance Resistance Potential fomite infestation Oral Ivermectin 200ug/kg Recommendation: Repeat tx after 1 week Fine combing of hair with nit comb Wet combing Increases yield by prying the adult lice from the hair follicle Occlusion and Suffocation Shaving one’s head to avoid infestation 6th century BC when priests and wealthy Egyptians shaved their hair and wore wigs Routine head shaving in military service WHO – read 24H after application otherwise mortality rates are overestimated Headlice have the ability to “resurrect” from a state of seeming death in which resp and motor fxn appear to have ceased. Less dependent on continuous nervous control of respiration and circulation. Pediculosis Humanus Humanus 2-4 mm; larger than head louse Attaches to body hair to feed Survive w/o blood meals up to 3 days Risk factors: poverty, war, natural disasters, refugee-camp populations Body lice transmit many infectious agents while feeding: - Bartonella Quintana (trench fever and endocarditis) - Rickettsia Prowazekii ( louse-borne relapsing fever) F lay eggs (270-300 ova) Nits (ova w/ chitinous case) Incubate for 8-10 days Life span: 18 days Nymphs mature to adults in 14 days Papular urticaria Changes secondary to rubbing and scratching (excoriations, eczema, LSC, infection, PIH) * scabies, pediculosis capitis and pulex irritans (human flea) can coexist (+) lice and nits in clothing seams (+) lice grab on body hairs to feed Atopic dermatitis Contact dermatitis Scabies Cutaneous drug reaction Decontamination of clothing and bedding Delousing ◦ Pyrethrin ◦ Permethrin ◦ Malathion Two types: 1. Cimex lectularius – temperate climate 2. Cimex hemipterus – tropical climate Flat, oval body Retroverted mouthparts for blood meals Breed through traumatic insemination ◦ Male punctures the female and deposit sperm into her body cavity Hide in cracks and crevices Infest bats and birds Suspected vectors for Chaga’s disease and Hepatitis B Can survive for 1 year without feeding but usually seek a blood meal q5-10 days Nocturnal feeder Attracted to the warmth and carbon dioxide production of their victim Complete their meal in a minute then return to hiding Spread in clothing & baggage of travelers, secondhand mattresses & laundry Painless Usually overlooked unless large numbers Multiple and grouped in a linear fashion Raw of 3 bedbug bite is referred to as breakfast, lunch and dinner Wheals and papules with small hemorrhagic punctum at the center Bullous reactions to sensitized individual Hypersensitivity to the reaction have been reported Drug Eruptions Ecthyma Insect Bites Pemphigus Herpetiformis Scabies Symptomatic tx of bites Local wound care Elimination of bird’s nest and bat roosts Cracks and crevices in the house should be eliminated and treated with insecticide Frequent retreatment may be necessary “SCIENTIA MAXIME CUM VIRTUTE” Knowledge is best with virtue