Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
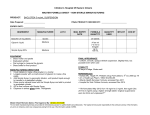
IMPROVING ADHERENCE TO MALARIA TREATMENT FOR CHILDREN: THE USE OF PRE-PACKAGED CHLOROQUINE TABLETS VRS. SYRUP EVELYN K. ANSAH, IRENE A. AGYEPONG, JOHN O. GYAPONG, DAVID B. EVANS Order of Presentation Background Study setting Methods Results Key lessons learnt Policy and Program Implications Conclusion Background Follow-on to initial study on adherence in the Dangme West District Adherence to Rx schedule was found to be very poor especially for chn (Agyepong et al,2002; Social Science & Medicine 2002 Dec ; 55(12): 2215-2226) Syrup mainstay of antimalarial Rx among chn <5 yrs Pre-packaged tablets for adults shown to improve adherence remarkably (Yeboah-Antwi et al, 2001,Quingjun et al, 1995) Study Setting Cape Coast municipality in the Central Region of Ghana Population: 120,000 2 H/Centers 2 MCH Centers Malaria is highly endemic; there is transmission all year round Research Questions Would prescribing pre-packaged tablets improve adherence to antimalarial Rx for children <5yrs? Would tablets be acceptable to mothers as an alternative formulation for children? Methods 144 clients randomly assigned to receive syrup, 155 to receive prepackaged tablets at OPD 1 2 3 Day 4 home visit. (The first day of visit to the clinic was counted as day 1) Methods Caregivers were interviewed to find out how medication was administered and their perceptions of the formulation received Volume of spoons/other home implements used to administer syrup measured using a calibrated measuring syringe Definition of Adherence used Doing exactly as the provider prescribed no matter the volume and type of implement used e.g Mother gives exactly “one teaspoon” daily even if her idea of a teaspoon is a tablespoon. Results 42% of 144 clients who received syrup c/f 91% of 155 who received pre-packaged tablets adhered to Rx schedule 80% used spoons whilst 20% used a small cup to measure the dose (Syrups were/still are dispensed at the clinic without a standard measure) Only 19.4% used an accurate 5 ml measure. 68% used measuring implements <5ml. The rest used implements >5ml in volume Results The volume of spoons/cups used to represent 5 mls varied from 1 ml to 9 mls. Some used teaspoons whilst others used dessertspoons and tablespoons. Apparently to most of the caregivers/ mothers, “a spoon is a tablespoon is a desertspoon is a teaspoon” 4 caregivers used two different measures at different times or on a different days. Results Only 8.6% of caregivers had given a total dose of 25mg/kg by day 4 > 25mg/kg - 44.3% < 25mg/kg - 47.1% Cost to the caregiver when syrup was dispensed was about 4x that of tablets GHC750(US$0.36) vrs GHC168 (US$0.08) Perceptions of Caregivers /Mothers “Tablets are easier to administer than the syrup. I just put it in thick ‘koko’ (fermented maize porridge).” “It is easier for me to remember how much to give. As for 1,2,3 anybody can read it” “The tablets work faster than syrups.” About 62% of caregivers/mothers who received pre-packaged tabs preferred it to the syrup Key Lessons Pre-packaged tabs for children are a viable alternative for home management of malaria. Improves adherence remarkably & reduces over & under dosage --->Toxicity or resistance Also improves the administration of the correct dose Key Lessons Eliminates problem of variations in home measures and the mother’s dilemma of “HOW MUCH?’ “HOW OFTEN?” “HOW LONG?” Reduces cost to caregiver/mother Caregivers/ mothers are willing to use them Policy/Program Implications Policy makers must consider using pre-packaged tabs for children. Manufacturers must be encouraged to produce already packaged, lower strength, sweeter tabs for children Where syrup MUST necessarily be dispensed, standard 5ml measures must be provided with the medication In that case, just enough syrup with allowance for spillage must be supplied Future Research Agenda Would adherence to dosage schedule of co-packaged tablets be the same as for single drug tablets? (Current move to combination therapy for malaria) Addition of standard measures to syrups: by how much would adherence be improved? How do we ensure that prescribers and chemical sellers/Pharmacies do dispense adequate doses of antimalarials Thank you for your attention!!!