Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
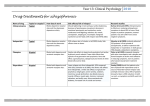
2007 ALCOHOL RELATED PROBLEMS Identification CAGE questionnaire Have you ever thought that you should Cut down on your drinking Has anyone Annoyed you by commenting on the amount you drink Have you ever felt Guilty about the amount you drink Do you ever have an Eye opener Cycle of change 1. Anger at mentioning alcohol Don’t pursue topic 2. Would like to change but not just yet Give written information about how to seek help 3. Wants to change now Use motivational interviewing technique to start change 4. Already started to change Reinforce and support change Barriers to change These need to be identified Motivational interviewing People believe what they hear themselves say Empathic interviewing style Open ended questions Reflective listening Get on their wavelength Feedback about risk Agree factual information about personal harm or impairment Balance sheet of pro’s and cons of changing /not changing Motivational interviewing People believe what they hear themselves say Roll with resistance Avoid confrontation Arguments about terms such as alcoholic are fruitless particularly in the early stages Support self efficacy Patient takes responsibility for achieving goals Choosing from menu of options Encourage belief that change is possible Motivational interviewing People believe what they hear themselves say Reinforce self motivate patients Recognition of harm caused Desire to change Feasibility of change Withdrawal symptoms Common features on stopping alcohol Anxiety and agitation Tachycardia Sweating Tremor of extended hands, tongue or eyelids Nausea and vomiting Insomnia Withdrawal fits Confusion hallucinations Withdrawal symptoms Should be mild if Alcohol free at consultation Male drinking < 15units/day Female drinking < 10 units/day Units of Alcohol 1 ordinary glass of wine ½ pint low strength beer 1 standard pub short 9/bottle Withdrawal symptoms Management – mild symptoms Rest Relaxation Reassurance that they will pass in a few days Explanation – they are evidence of that the brain has adapted to living in an alcoholic environment and will take time to readjust to one that is alcohol free Withdrawal symptoms Need for specialist or hospital referral Confusion Hallucinations History of fits or epilepsy Risk of suicide Failed home detox Poor nutrition Unsupportive home environment Acute physical or psychiatric illness Any symptoms of encepalopathy Wernicke’s encepalopathy Signs Confusion Ataxia Opthalmoplegia Nystagmus Coma Hypotension Hypothermia Any unexplained neuro signs during withdrawal Wernicke’s encepalopathy Require urgent specialist assessment Urgent treatment with parentral thiamine (Pabrinex IM ) Drug treatment Drug of choice for withdrawal are benzodiazepines Can induce temporary problems with cognition and recall Are addictive if taken over time Detox with benzos should not be continued for more than 7 days Start with high dose chlordiazepoxide 120mg/day or diazepam 20mg/day Detoxification regimen Ritson, B. BMJ 2005;330:139-141 Copyright ©2005 BMJ Publishing Group Ltd. Other support Patients and family should be advised To stay off work Not drive Rest Drink plenty of fluids – fruit juice rather than stimulants such as cafeine Abstain from alcohol Other support Community nurse of GP should visit daily to Monitor progress Review drugs Assess mental state and vital signs Breathalyse for alcohol if possible Patient may think they can now handle alcohol must make it clear that drinking must not be resumed Daily check Tremor Pulse Temperature Blood pressure Level of consciousness Orientation Dehydration Vitamins If well nourished with moderate alcohol dependence no vitamins required If under nourished or frequent relapse or self neglect Then 200-300mg thiamine a day for 2-3 months will help minimise risk to brain and peripheral nervous system May need parental admin during early stages of detox Preventing relapse Triggers to relapse Environment Availability Pub atmosphere Custom Always drinks at certain times, occasions and situations Interpersonal Stress conflicts Preventing relapse Triggers Intrapsychic Expectations Anxiety Social phobias Depression or elation Overconfidence Feeling good I have got over my drinking problem I can take some alcohol again Preventing relapse Drinking diary Balance sheet of good and bad consequences of continued drinking Patient should set own goals Monitor progress Identify ways of dealing with triggers to relapse Preventing relapse Pharmacotherapy Disulfiram Blocks metabolism of alcohol flooding the body with toxic acetaldehyde which causes flushing, palpitations, nausea, faintness and even collapse Start with 200mg/day can be increased to 400mg Contra indicated with liver disease, cardiovascular disorders, pregnant women, suicidal patients or those who are cognitively impaired Only effective if use is supervised Preventing relapse Pharmacotherapy Acamprosate Helpful adjunct to psychological therapies. Start as soon as abstinence is achieved Can be continued during relapse can be continued for 1 year Preventing relapse Drug treatments should always be accompanied by psychological support and therapy aimed at attaining a longer term change of lifestyle that is drug free