Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
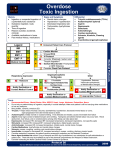
Toxicology Thomas Perera MD Toxicology What • • • • • is it? Poisonings Overdoses Side affects Exaggerated affects Exposures General Poisoning-The generally predictable and dose dependent effects of exposure to a potentially lethal substance. • • • • Almost anything is toxic if one uses enough Seen most in adults alcohol-crack-opioid Kids will put anything in their mouth Toxicology is not just ingestion but also inhaled, splashed, irradiated General • 2 million poisonings reported to tox centers per year – about 7% of ER visits • • • • • • 92% at home 94%single agent peak between 5pm-9pm 62% kids 88% accidental 7% with clear suicidal intent – 23% kids 13-17yrs • with adults fewer ingestion's but 82% intentional and accounting for 94% of deaths (total rate 1 in 300 attempts) General This is on of the areas where one can make a great impact • • • • Need for immediate therapy Acute action can save life Few areas like this Potential saves(narcan, oxygen) Where to start What we don’t have. • Exact information • patient-doctor bond • Time – extensive tests – gathering all necessary info • Cures for all toxins Where to start What we do have • Some history – EMS, Family, ID bracelets, patient’s account • Physical exam • Some quick tests • Some cures? Where to start A-airway B-breathing C-circulation • Now what? Toxidromes a common group of signs and symptoms which are associated with an overdose Toxidromes Opioid (5% of calls to poison control centers) • Depressed respiration -(Number and depth) – Due to loss of co2 drive stimulate remind to breath • • • • • Small-pinpoint pupils (parasympathetic) Decreased level of consciousness Hypotension Decreased bowel sounds Urinary retention Toxidromes Opioid • Also can have – pulmonary edema – hypoglycemia(not eating) – flushed skin – urticaria Examples:Herion, lomotil, etc. Demerol, Codeine, Toxidromes Sympathomimetics -fight or flight – stimulants- a drug that effects one or more organ system to produce an excitatory arousing effect, increased physical activity and vivaciousness and a promotes a sense of well being. Toxidromes Sympathomimetics -fight or flight • • • • • • dilated pupils sweating Increased HR, RR, BP dilated bronchi (epi does this) decreased bowel sounds, urine increased mental activity, reflexes, psychosis Toxidromes Sympathomimetics • Also can – pulmonary edema – seizures – focal neurologic changes Cocaine Not thought to be drug of abuse until 1970 • purer forms • increased popularity Many forms same effects but onset and duration vary • cocaine burns when lit but when changed to free base-crack • onset related to rush Cocaine Rout Inhaled7sec IV nasal oral onset peak 1-5min 15sec 3min 10min duration 20min 3-5min 15min 60min 20-30min 45-90min 60min Cocaine Chest pain ?antidote • dog study in 80’s – – – – – increased vitals seizures increased agitation increased temp death Toxidromes Anticholinergic(atropine,scopolamine,Benadryl,cogentin, flexeril,nightshade, jimson weed) • • • • • • • warm dry psychotic flushed decreased bowel sounds urinary retention dilated pupils Toxidromes Anticholinergic • ?cure -physostigmine Examples: • Atropine,Scopolamine • Benadryl, Cogentin • Flexeril • nightshade, jimson weed cyclic antidepressants uses in depression, chronic pain, enuresis, insomnia toxic manifestation • As anticholinergic • CNS depression • Cardiac tox – Disrhythmia: Many types cyclic antidepressants treatment • • • • No physostigmine--seizures Cardiac -Na channel block-type 1a- no procaine agitation no haldol seizure-even valium not great Toxidromes Cholinergic--pesticides, serin gas • S alivation • L acrimation • U rination • D efication • G astric irritation • E mesis Also-small pupils, confusion, pulmonary edema. bardycardia, seizures Toxidromes Cholinergic • Cure -- atropine Toxidromes Sedative • • • • • • Hypnotic normal pupils (unless hypoxic) decreased respiration flaccid tone hypotension hypothermia Skin-vesicles on errythematous base Toxidromes Sedative Hypnotic • Cure - supportive measures – intubate early Toxidromes Hallucinogens • behavioral changes • altered perception • tachy,hypertesive,large pupils, tremor, piloerrection, hyperthermia Toxidromes Hallucinogens • PCP – Like cocaine but with hallucinations • nystagmus – Complications • Rhabdo, hypertension, seizures, hypoglycemia, bronchospasm Cocktail-Coma/AMS Oxygen-always • Tox patients usually younger low likelihood of COPD so do not worry about decreased CO2 drive • Opioids-stimulate respiration- sometimes only need to remind to breath even if apnic. • watch out for vomiting in to mask Cocktail-Coma/AMS Glucose • its use based on the number of times AMS caused by hypoglycemia(can do anything) • Also hypoglycemia can accompany toxic exposure – Hyperactivity, seizure etc.-uses up glucose stores – Drug users not well nourished – Alcoholics with bad livers – Children also with decreased stores Cocktail-Coma/AMS Glucose • Potential risk of worsening stroke – risk benefit – presentation – different disease Cocktail-Coma/AMS Thiamin • given on theoretical ground that glucose load can precipitate Wernickes • No down side • Side note Cocktail-Coma/AMS Narcan-Naloxone HCL • competitive antagonist • IV, IM, ET, SQ, SL, PO • good for many opioids but not all – methadone, pentazosine, propoxyphene, Demerol – initial dose 2mg if response or high suspicion more Cocktail-Coma/AMS Narcan • very safe(large doses for body packers) • short lived • downside – withdrawal-vomiting, agitation, abdominal pain, sweating, diarrhea, piloerrection – unmasking co-ingestion Cocktail-Coma/AMS no physostigmine no ipecac • • • • delayed charcoal ruptured esophagus Mallory-Wise aspiration Treating complications Hypotension • Fluid, fluid, fluid • pressers not dopamine-levaphed Hyperthermia • cooling • decrease agitation Treating complications Agitation • benzodiazapine • hypoxia, glucose, etc. Treating complications seizures • Benzodiazipine • not dilantin-interacts with to many drugs wrong mechanism • hx important -INH-pyridoxine Treating complications Arrhythmia-protocol • • • • • mostly sinus tach deal with hypoxia, agitation, etc. tricyclic-bicarb--not procaine dig-avoid Ca-dilantin B Blocker, Ca channel Blocker-glucagon Other stuff Protect Hx yourself what, how, when consider associated trauma Intubate early