Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
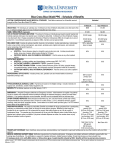
PPO PLAN GEORGIA IN-NETWORK Plan Vendor:1st Medical Network DEDUCTIBLE $300 PER PERSON $900 PER FAMILY $20 COPAY FOR OFFICE VISITS (not subject to general deductible) $750 per person Wellness Care STOP LOSS: $1,000/person $2,000/family PPO PLAN NATIONAL IN-NETWORK Plan Vendor: Beech Street DEDUCTIBLE $400 PER PERSON $1,200 PER FAMILY $20 COPAY FOR OFFICE VISITS (not subject to general deductible) $750 per person Wellness Care STOP LOSS: $2,000/person $4,000/family PPO PLAN OUT-OF-NETWORK DEDUCTIBLE $400 PER PERSON $1,200 PER FAMILY %60 of network rate for most of the services SUBJECT TO DEDUCTIBLE AND BALANCE BILLING PHARMACY PROGRAM Network of Retail Pharmacies Services Outside of Network 90 Day Maximum Drug Supply $10 co-payment for generic $25 co-payment for preferred brand name 20% of non-preferred brand name cost ($40 min. and $100 max.) VISION CARE PROGRAM BLUE CHOICE VISION PROVIDERS LensCrafters Independent Optometrists Independent Ophthalmologists VISION DISCOUNTS LensCrafters Preset Vision Packages ~Silver, Gold, and Blue Choices~ 30% Off Eyeglasses/Frames/Lenses/Lab Fees 25% Off Non-Prescription Sunglasses Low Fixed Prices on Contact Lenses PPO PLAN MEDCALL emergency room copayment: $75 reduced to $50 if referred by MedCall Copayment fully waived if admitted. PPO PLAN COST PER MONTH -Employee $105.18 -Employee/Spouse $220.84 -Employee/Child $189.30 -Family $304.96