Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
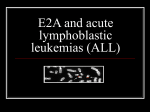
Independent review of the circumstances surrounding four serious adverse incidents that occurred in the Oncology Day Beds Unit, Bristol Royal Hospital for Children on Wednesday, 3 January 2007 Jonathan Sheffield Medical Director All HUMAN BEINGS ARE PRONE TO MAKING INADVERTANT ERRORS Heparin. Summary: incidents aetiology • • • • • • • The security status of the Controlled Drugs Cabinet in which the CPA’s drugs were stored appears to have been cognitively down graded from high security to a safe place to keep things. CPA was in a rush to start the List. He had not been able to have a rest break and had recently been given some distressing news. CPA was not aware that monoparin was stored in the CDC. CPA had seen the drug that he intended to use to keep the patients intravenous catheters and cannula patent (Hepsal) unboxed in the CDC on previous occasions. CPA did not read the labels on the ampoules of monoparin correctly, i.e. he saw what he expected to see rather than perceiving the information that was physically present. CPA undertook the preparation of the drugs for all four patients in one batch thus creating the potential for a systemic failure which then occurred. CPA did not carry out a verbal double-checking safety protocol because he was not aware that the Trusts Medicines Code required him to undertake one before the administration of medicines to children. Comparison outer packaging monoparin and Hepsal Comparison monoparin and Hepsal ampoules respectively Hepsal and monoparin ampoules respectively The incident • What, when, how and who? • Site visit • Decision Families • How • Why • Future Why independent? • Objectivity • Open • Change Previous knowledge • • • • • • Human beings are prone to making inadvertent errors and especially when working conditions are less than optimum It is well known that look-alike drug labels have led to patients being harmed inadvertently by healthcare professionals Patients prescribed ‘heparin flushes’ have on numerous occasions been inadvertently administered significant overdoses of heparin e.g. USA September 2006 Latest incident - USA 21 November 2007, Denis Quaid twins plus two other neonates 1000 times more heparin than intended Verbal double safety checks can reduce the risk of an error being made e.g. radiotherapy, IVF or airline pilots cross checks Batch working can lead to systemic failures Trust outcome • Go to action plan