Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
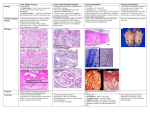
ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal 30.7.09 (9.00 pm) Same patient next day morning CAUSES COPD-acute exacerbations Pulmonary oedema Pneumo-thorax Br. asthma Pneumonia Pulmonary Embolism Anaphylactic reaction Acute Laryngeal Obstruction a. oedema b. Foreign body Anxiety Neurosis Difference between cardiac asthma and COPD History Hypertension or valvular S/O of COPD or asthma heart diseases Clinical examination High B.P. Pulsus alternans C/F of LVH Predominant basal crepts Pulsus paradoxus C/F of emphysema Predominant expiratory rhonchi (wheeze) Pulmonary oedema . Cardiogenic -LV failure due to Myocardial infarction, ventricular septal rupture following infarction Valvular: acute aortic regurgitation, acute mitral regurgitation, severe aortic stenosis Severe hypertension Acute arrhythmia Acute myocarditis Acute volume overload Cardiomyopathy Why the patient with pulmonary oedema is breathless ? Non Cardiogenic . Increased pulmonary capillary permeability Acute respiratory distress syndrome (ARDS) -PAWP < 18 mm International criteria 1. Acute onset of symptoms 2. The ratio of the arterial partial pressure of oxygen (PaO2) to the fraction of inspired oxygen (FIO2) of 200 mm Hg or less For Example normal PaO2 = 100, FiO2 = 20% or 1/5 so the above ratio = 100/1/5 = 500 mm Hg 3.Bilateral infiltrates on CXRs 4.Pulmonary arterial wedge pressure of 18 mm Hg or less or no clinical signs of left atrial hypertension causes of mediator release leading to ARDS Sepsis/pneumonia • secondary risk factors alcoholism cigarette smoking Gastric aspiration lung trauma due to smoke inhalation fat emboli direct effects of large amounts of necrotic tissue Less common causes Post-bone marrow transplant Drug overdose - tricyclic antidepressants, opiates, cocaine, aspirin Near drowning Following upper airway obstruction; mechanism unclear Acute form of Interstitial Pneumonia. Also known as acute Hamman-Rich syndrome Indirect (non-pulmonary) injury Shock Septicaemia Amniotic or fat embolism Acute pancreatitis Massive haemorrhage Multiple transfusions DIC Massive burns Major trauma Head injury • Raised ICP • Intracranial bleed Cardio-pulmonary bypass Acute liver failure . airway obstruction laryngeal obstruction tumor infections oedema foreign body What is the most charecteristic feature of laryngeal obstruction ? . Coronary artery disease -May present without chest pain “anginal equivalent” Pulmonary embolism Venous stasis -immobility endothelial damage recent trauma surgery burns indwelling catheters IV drug use. hypercoagulability malignancy obesity pregnancy HRT/OCP BTS pre-test clinical probability scoring Patient has clinical features compatible with PE: • raised respiratory rate • ± haemoptysis • ± pleuritic chest pain. Plus 2 other factors: • 1. Absence of another reasonable clinical explanation • 2. Presence of a major risk factor A. plus 1 and 2: HIGH pre-test clinical probability A. plus 1 or 2: INTERMEDIATE pre-test clinical probability A. alone: LOW pre-test clinical probability Severity of Br. Asthma Symptoms noct. Sympt • Stage 4 Continuous Frequent Severe • Stage 3 Daily Moderate • Stage 2 Mild >1 /week but <1time/day >1 time /week >2 times a month • Stage 1 <1 time /week <2 times Intermittent a month FEV1/PEFR <60% predicted variability >30% 60-80% predicted variability >30% >80% predicted variability 20-30% >80% predicted severe Asthma Life-threatening asthma Near-fatal asthma severe Asthma PEF 30- 50% best or predicted Respiratory rate >25/min Tachycardia: heart rate >100/min Inability to complete sentences in one breath Life-threatening asthma Severe airways obstruction •PEF <33% best or predicted •Soft breath sounds or silent chest •Feeble respiratory effort Increased work of breathing & haemodynamic stress •Exhaustion •Hypotension (systolic BP <100mmHg) Ventilation-perfusion mismatch •Cyanosis •Hypoxia (SpO2 <92% and/or PaO2 50mm irrespective of inspired O2 concentration) Ventilatory failure •Rising PaCO2 •Confusion or coma Near-fatal asthma Raised PaCO2 immediate requirement for ventilation with raised inflation pressures Management Oxygen Oxygen is the primary therapeutic modality -corrects V/Q mismatch. -provided via nasal cannula or face masks In significant hypoxemia nonrebreathing masks may be used to deliver as much as 98% oxygen Goal of supplemental oxygen therapy is an oxygen saturation above 92% Non rebreathing mask Inhaled beta-agonists Salbutamol Albuterol & Levalbuterol Terbutaline • • • • mainstays of acute therapy in asthma. They act via stimulation of cyclic (AMP)– mediated bronchodilation. stimulation of receptors relaxes airway smooth muscles increases mucociliary clearance & decreases mucous production. Anticholinergics act via inhibition of cyclic guanosine monophosphate (GMP)–mediated bronchoconstriction. -decrease mucus production -improve mucociliary clearance Ipratropium bromide -agent of choice. In severe airflow obstruction - combination of ipratropium and salbutamol/albuterol provide better broncho dilatation than used alone. Corticosteroids Hydrocortisone Methylprednisolone decrease airway inflammation and swelling. potentiate the effects of beta-agonist agents improve capillary leak. administered intravenously or orally. -Used mostly I.V.during status asthmaticus Further therapy Magnesium sulphate Magnesium can relax smooth muscle and hence cause bronchodilation by competing with calcium at calciummediated smooth muscle binding sites. The published doses used range from 2575 mg/kg infused over 20 minutes, with a maximum of 2-2.5 g/dose. Intravenous beta-agonists patients with refractory status asthmaticus may respond to intravenous administration of beta-agonists. . • Intravenous terbutaline albuterol or salbutamol. i.v. terbutaline 0.4 - 10 mcg/kg/min • dose administered should be titrated to effect and adverse cardiac effects (tachycardia, arrhythmias, hypokalemia) monitoring of cardiac enzyme levels in patients receiving prolonged intravenous beta-agonists Ketamine Ketamine is a short-acting pentachlorophenol (PCP) derivative bronchodilatory effects increases endogenous catecholamine levels Acts as a sedative to reduce anxiety and agitation that can exacerbate tachypnea and work of breathing useful in small children with status asthmaticus . Methylxanthines . role of methylxanthines -Theophylline or Aminophylline(theophylline & ethylenediamine in 2:1 ratio) is now debated. have many undesirable adverse effects, such as nausea and vomiting. studies have failed to show additional benefit when methylxanthines are administered to patients who are already receiving frequent beta-agonists and steroids • recent studies have examined methylxanthines theophylline and aminophylline and demonstrated improvement in the clinical asthma scores when compared with placebo control. The theophylline effects are • bronchodilatation, • increased diaphragmatic function • central stimulation of breathing Continuous positive airway pressure (CPAP) Indications for intubation and mechanical ventilation . Apnea or respiratory arrest Diminishing level of consciousness Impending respiratory failure marked by significantly rising PCO2 with fatigue decreased air movement altered level of consciousness Significant hypoxemia that is poorly responsive or unresponsive to supplemental oxygen therapy alone Considerations in mechanical ventilation • Positive pressure ventilation in asthma Complicated by severe airway obstruction & air trapping resulting in hyperinflated lungs resisting further inflation & places patient at high risk of barotrauma • mechanical ventilation should be undertaken only in the face of continued deterioration despite maximal broncho dilatory therapy • prolongation of the time needed for lung units to fill and empty. • Slow ventilator rates are usually needed • principle of mechanical ventilation of status asthmaticus is controlled hypoventilation, tolerating higher levels of PCO2 in order to minimize tidal volume and peak inspiratory pressures . • Permissive hypercapnia can be tolerated as long as the patient remains adequately oxygenated Tension pneumothorax Emergent needle decompression Administer 100% oxygen, and ventilate if necessary Locate anatomic landmarks and quickly prepare the area to be punctured with an iodine-based solution (eg, Betadine) Insert a large-bore (ie, 14-gauge or 16gauge) needle with a catheter into the second intercostal space, just superior to the third rib at the midclavicular line, 1-2 cm from the sternal edge (to avoid injury to the internal thoracic artery) Use a 3-6 cm long needle, and hold it perpendicular to the chest wall when inserting Once the needle is in the pleural space, listen for the hissing sound of air escaping and remove the needle while leaving the catheter in place Secure the catheter in place, and install a flutter valve Prepare the patient for tube thoracostomy. Tube thoracostomy • Tube thoracostomy is the definitive treatment fortension pneumothorax • needle decompression followed up immediate with tube thoracostomy • hemothorax along with tension pneumothorax is common • Monitor the patient continuously for arterial oxygen saturation Comparison COPD Vs Br. Asthma airflow obstruction due Chronic obstruction of to inflammation & lung airflow which is increased airway permanent & hyper-responsive ness progressive over time & bronchospasm which is variable over short periods of time reversible with treatment cause Mostly by allergens in Due to the chemical atopic persons irritation of the airways caused by smoke(ing) Age group Mostly affects the young people Disease of middle aged & elderly Pathogenesis Airway obstruction due to Due to • Smooth muscle spasm • oedema • Loss of elastic recoil • Remodeling of the air way Clinical features Chest normal in between the attacks Features of air way obstruction always seen Complications Emphysematous changes do not occur Does not progress to cor pulmonale or type II respiratory failure Seen after some years Many cases develop these complication Pulmonary Function Test Obstructive picture + 1. FEV1 ≥ 15% (and 200 ml) increase following administration of a bronchodilator/trial of corticosteroids 2. > 20% diurnal variation on ≥ 3 days in a week for 2 weeks on PEF diary 3. FEV1 ≥ 15% decrease after 6 mins of exercise Obstructive pattern + 1. Minimal bronchodilator reversibility (<15%, usually <10%) 2. < 20% diurnal variation on ≥ 3 days in a week for 2 weeks on PEF diary No change in FEV1: FVC with exercise (absence of exercise induced bronchospasm) 3. X ray chest Normal in between attacks. Hyper inflated lungs at the time of acute attack Shows • • Emphysematous changes with bullae Features of pulmonary hypertension Hoover's sign refers to the inspiratory retraction of the lower intercostal spaces results from alteration in dynamics of diaphragmatic contraction due to hyperinflation resulting in traction on the rib margins by the flattened diaphragm Seen in up to 70% of patients with severe obstruction can be an excellent marker for severe airway obstruction