Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
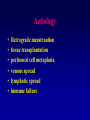
The Modern Management of Endometriosis Malcolm Padwick What is it ? The presence of endometrial tissue outside of the uterine cavity • cul-de-sac • rectovaginal septum • surface of rectum • fallopian tubes and ovaries • uterosacral ligaments • bladder • pelvic side wall Is it inherited? • 6 to 8 fold increase risk in sisters compared to unrelated women • affected sisters are more likely to have severe disease • OXEGENE study ongoing • ovarian cancer link • racial Aetiology • • • • • • Retrograde menstruation tissue transplantation peritoneal cell metaplasia venous spread lymphatic spread immune failure Incidence • At sterilisation 2 to 5 % have endometriosis • 25 to 50 % of women investigated for infertility • estimated 5 million women in USA • 6 to 7 % of all females Endometriosis symptoms dysmenorrhoea pelvic pain infertility dyspareunia menstrual irregularities other cyclic bleeding 70% 40% 35% 33% 15% 1-2% Endometriosis Diagnosis • laparoscopy The natural progression Lesions Clear Red Black mean age 21.5 mean age 31.9 disease is progressive in 47 - 64% of women and in 20% of treated women (Redwine) Endometriosis and Fertility • 30 to 40 % of women with endometriosis are infertile • may be obvious anatomical abnormalities • hormonal E2 reduced LH blunted • multicystic ovaries • Luteinized Unruptured Follicle X 3 • peritoneal fluid, macrophages, cytokines, interferon C3, C4 are all increased • plasma embryotoxic in 78% of cases Endometriosis Management options 1 Diagnostic laparoscopy Drugs • OCP • Provera • Danazol / Gestrinone • GNRH analogues Surgery • Hysterectomy with BSO Endometriosis and Fertility Hormonal or antihormonal therapy has no beneficial effect on fertility either alone or as an adjunct to surgery ( RCOG recommendation) only surgical ablation or excision of disease will restore fertility ( RCOG recommendation) Endometriosis Management option 2 • Diagnostic laparoscopy proceeding to immediate corrective surgery; LASER and /or laparoscopic resection of diseased tissue Endometriosis CO 2 LASER Vs Diathermy • • • • • depth of destruction accuracy collateral / unseen damage placebo effect cost Pelvic side wall Endometriosis Treatment by CO2 LASER Classification Pregnancies Improved pain I minimal II mild III moderate IV severe 72% 60% 50% 44% 89% 87% 85% 80% AFS Del Pozo 1997 Women with pain • Drug therapy may relieve inflammation and reduce pain in early superficial disease but corrective surgery +/- drug therapy is preferable (Padwick 1999) • rectovaginal, rectal and uterosacral lesions always need surgery • endometriomas always need surgery • abnormal anatomy and adhesions always need surgery Rectal involvement Endometriosis on the caecum Endometriosis on the caecum Endometrioma LASER ablation of endometriosis • endometriosis not cured by medication • surgery may cure the younger woman Techniques • ablate • LUNA • resect peritoneum • ventrosuspension Before After But what if ? Requirements • full RCOG accreditation • MAS accreditation – surgeon – preceptor – LASER certification What to expect • • • • • • Overnight stay (98%) 3 puncture marks 5mm in length Voltarol / oral analgesics 1 to 2 weeks off work Mostly an immediate difference in pains Benefits of fertility are immediate West Herts Audit • • • • • • • 150 + women treated per year > 500 women treated > 95% diagnostic rate No acute complications No laparotomies One late sepsis Outcome measures ?? Conclusion Endometriosis should be treated early and aggressively by surgical destruction or excision, ideally at laparoscopy. Drug therapy which is expensive, largely ineffective and has significant side-effects should be reserved for selected cases requiring post surgical maintenance therapy. Padwick 1999