Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
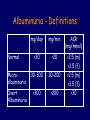
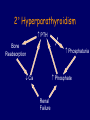
Derby Nephrology Research Management of Chronic Kidney Disease in Primary Care Maarten Taal Consultant Renal Physician Derby City General Hospital Topics • • • • • • CKD Classification Estimated GFR Proteinuria Slowing CKD progression Cardiovascular Risk in CKD Complications of CKD – anaemia and bone disease • Drugs in CKD • CKD in Primary Care and when to Refer • Renal Risk in Derby (R2ID) Study Prevalence of CKD: NHANES 1999-2004 CKD 5 0.4% CKD 4 CKD 3 5.4% CKD 2 5.4% CKD 1 5.7% Total 16.8% n=12,785 MMWR Morb Mortal Wkly Rep. 56:161; 2007 CKD Prevalence in the UK • NEOERICA • CKD stage 3-5 among 130,226 patients registered with GPs in Kent, Manchester and Surrey • Age-standardized prevalence: males: 5.8% females: 10.6% Stevens PE et al. KI 72:92; 2007 Measurement of renal function Glomerular filtration rate • The GFR (commonly expressed as mL/min) is a measure of the blood volume filtered by the kidney • Accurate measurement is important for assessment of the severity of renal disease Common clinical measures • Serum creatinine – Creatinine metabolite of creatine in skeletal muscle – Tubular excretion in proximal tubule (i.e. not all is from passive filtration) – Concentration dependant on renal function, diet, muscle mass, age, gender, ethnic background), affected by some drugs – NICE recommends 12h meat fast Serum creatinine • Advantages – Simple to carry out – Cheap – Good serial measure • Disadvantages – Not accurate measure of GFR – Non-linear relationship to GFR Abnormal renal function Creatinine clearance • Combining urinary clearance and serum creatinine – – – – GFR = U x V / P U = urinary concentration V = urinary volume P = plasma concentration Creatinine clearance • Advantages – More accurate than serum creatinine – Combine with other tests (e.g protein) • Disadvantages – – – – Costly Inconvenient Subject error Secretion of creatinine is dependent on renal function – Not corrected for body surface area Formulae to estimate GFR • Cockcroft-Gault – not corrected for BSA – (140-age) *LBW (kg) *1.22 / S Cr (umol/L) (male) – (140-age) *LBW (kg) *1.04 / S Cr (umol/L) (female) • Modified MDRD – corrected for BSA – 2.59 x ((serum creatinine (umol/L)) exp[-1.154]) x (Age exp[-0.203]) x (0.742 if female) x (1.21 if African American) Estimated GFR MDRD formula: 2.59 x ((serum creatinine (umol/L)) exp[-1.154]) x (age exp[-0.203]) x (0.742 if female) x (1.21 if African American) Copyright ©2007 BMJ Publishing Group Ltd. Giles, P. D et al. BMJ 334:1198-1200; 2007 MDRD formula: Limitations • Underestimates GFR for values >60ml/min • Variation in creatinine assays • Not adequately validated in: – Ethnic groups other than African American – Elderly – Extremes of body habitus MDRD Formula: Solutions • Standardise creatinine assays (National External Quality Assurance Scheme) • Modification of formula • Do not report eGFR if >60ml/min • Creatinine clearance or isotope GFR if GFR>60 • Validation in different ethnic groups • New formulae • New markers – cystatin C Proteinuria – detection and monitoring • Dipstick potentially misleading • Albuminuria vs. Proteinuria Albuminuria - Definitions mg/day mg/min ACR (mg/mmol) <30 <20 Microalbuminuria 30-300 20-200 Overt Albuminuria >300 >200 <2.5 (m) <3.5 (f) >2.5 (m) >3.5 (f) >30 Normal Proteinuria - Definitions g/day mg/mg mg/mmol Normal <0.15 <0.2 <20 Mild 0.15-1.0 0.2-1.0 20-100 Moderate 1.0-3.5 1.0-3.5 100-350 Severe/ >3.5 Nephrotic >3.5 >350 CKD Management Goals • Slow progression of CKD • Reduce Cardiovascular Risk • Detect and treat complications of CKD – Ca and phosphate – Anaemia • Avoid drug toxicity • Appropriate referral CKD Progression 0.008 0.007 FSGS 1/creatinine 0.006 0.005 0.004 0.003 0.002 Hypertension Proteinuria 0.001 0 0 6 12 18 24 30 36 time (months) 42 48 54 60 CKD Progression - 2009 Systemic Hypertension Pgc SNGFR 1°Renal Disease Mechanical Stress Nephron Loss Ang II Proteinuria Macrophages Fibroblasts 2° FSGS and TIF TGF- Cytokines CAMs Interventions for Slowing CKD Progression • • • • • Lower BP to <130/80mmHg ACEI or ARB as first line Minimise proteinuria (<1g/day) Weight loss if obese Smoking cessation Interventions to Slow CKD Progression Systemic Hypertension Pgc SNGFR 1°Renal Disease Treat Hypertension Weight loss Dietary Protein Mechanical Stress Nephron Loss Inhibit RAS Ang II Proteinuria Treat Dyslipidaemia Stop Smoking 2° FSGS and TIF Macrophages Fibroblasts New Anti-inflammatory Anti-fibrotic Proteinuria TGF- Cytokines CAMs CV Risk in CKD Age-Standardized Rates of Cardiovascular Events According to the Estimated GFR among 1,120,295 Ambulatory Adults Go, A. S. et al. NEJM 2004;351:1296-1305 Reducing CV Risk in CKD • • • • • • Control hypertension (<130/80mmHg) ACEI or ARB as first choice Treat dyslipidemia as for “high risk” Smoking cessation Aspirin for diabetics and ?others Ca and phosphate control Vitamin D Metabolism UV light 7-dehydrocholesterol Diet Cholecalciferol Liver 25OH-Cholecalciferol Kidney Prox Tubule Cells Ca absorption in Small intestine 1,25OH-Cholecalciferol Calcium and Phosphate in CKD • Failure of 1-hydroxylation of vitamin D results in decreased intestinal Ca absorption hypocalcaemia • Failure of renal phosphate excretion hyperphosphataemia 2° Hyperparathyroidism PTH Bone Reabsorption Phosphaturia Ca Phosphate Renal Failure Consequences of Ca / P and PTH Abnormalities • Renal Osteodystrophy – High turn-over: Osteitis fibrosa cystica – Low turn-over: Adynamic bone disease • Vascular calcification • Increased mortality • Other PTH effects – response to epoetins – immune response Mean Coronary Calcium Score Coronary Calcification 2500 No CAD CAD Dialysis 2000 1500 1000 500 0 28-39 40-49 50-59 60-69 Age (years) Adapted from Braun J et al. Am J Kid Dis. 1996;27:394-401. Ca x P and Survival on HD 1.2 1.0 .8 .6 Ca x P >5.50 .4 5.00-5.49 3.65-4.99 .2 -200 <3.64 0 200 400 600 800 Survival (days) 1000 1200 1400 Taal et al. Kidney Int 2003 Management of Ca /P Abn • Phosphate control – Dietary restriction – Phosphate binders (CaCO3, Ca acetate, AlOH sevelamer, lanthanum) • 1- cholecalciferol replacement – Increases intestinal Ca absorption – Directly suppresses parathyroids • Calcimimetics (cinacalcet) – Modulate calcium sensing receptor Erythropoietin • EPO = main regulator of normal erythropoiesis • Primary source of EPO = kidney (90%) • Primary site of EPO production = renal peritubular capillary endothelial cells ± interstitial fibroblasts • Tissue hypoxia EPO Anaemia in CKD • Is an important contributor to symptoms of CRF: – – – – Tiredness and lethargy Dyspnoea Poor concentration /Memory Anorexia • Typically normochromic, normocytic • Due primarily to deficient renal production of erythropoietin Anaemia management in CKD • • • • • Correct iron deficiency (IV iron) Treat inflammation Treat hyperparathyroidism Recombinant Epoetins – s.c. or i.v. Target haemoglobin 10.5-12.5g/dl Drug Toxicity in CKD • • • • • • NSAIDs K-sparing diuretics Trimethoprim Metformin (avoid in GFR<40ml/min) Gabapentin; Pregabalin Opiates ACEI or ARB in CKD - safety Creatinine rise • Predicts greater renoprotective efficacy • Allow up to 30% if not progressive • Contraindicated in bilateral RAS • Omit diuretics for 1-2 days • Avoid NSAIDs • Start low dose • Check serum creatinine at 1 week ACEI or ARB in CKD - safety Hyperkalaemia • Incidence of uncontrolled hyperkalaemia 0-4% in 6 large studies • Dietary advice • Avoid K-sparing diuretics High Potassium Foods • • • • • • Bananas, Oranges, Strawberries Tomatoes, Sprouts Jacket Potatoes, Chips, Crisps Coffee, Chocolate, Nuts Beer, Wine “Lo-Salt” Chronic diseases with cardiovascular component • Diabetes – – – – Lifestyle Blood pressure Cardiovascular risk Glycaemic control • CKD – – – – Lifestyle Blood pressure Cardiovascular risk Specific measures • IHD and Cerebrovascular – Lifestyle – Blood pressure – Cholesterol Quality and Outcomes Framework • CKD 3-5 register • CKD BP recorded • CKD BP<140/85 • CKD+HT on ACEI/ARB • DM BP recorded • DM BP<145/85 • DM screen for albuminuria • DM+albuminuria on ACEI/ARB • DM eGFR/creatinine checked Total 6 6 11 4 3 17 3 3 3 56 (1000) When to refer – stage 4 and 5 CKD (with or without diabetes) – higher levels of proteinuria (ACR ≥ 70 mg/mmol, PCR ≥ 100 mg/mmol, or urinary protein excretion ≥ 1 g/24 h) unless known to be due to diabetes and already appropriately treated – proteinuria (ACR ≥ 30 mg/mmol, PCR ≥ 50 mg/mmol, or urinary protein excretion ≥ 0.5 g/24 h) together with haematuria – rapidly declining eGFR (> 5 ml/min/1.73 m2 in 1 year, or > 10 ml/min/1.73 m2 within 5 years) – hypertension - poorly controlled despite the use of at least four antihypertensive drugs at therapeutic doses – people with, or suspected of having, rare or genetic causes of CKD – suspected renal artery stenosis Who to Test for CKD – diabetes – hypertension – cardiovascular disease (ischaemic heart disease, chronic heart failure, peripheral vascular disease and cerebral vascular disease) – structural renal tract disease, renal calculi or prostatic hypertrophy – multisystem diseases with potential kidney involvement – for example, systemic lupus erythematosus – family history of stage 5 CKD or hereditary kidney disease – opportunistic detection of haematuria or proteinuria. www.derby-cvsuccesszone.co.uk Renal Risk in Derby (R2ID) Study • Cohort study of patients with CKD 3 • Based in Primary Care • Important unanswered questions: – – – – – Characteristics of patients on CKD registers? Risk of GFR decline in individual patients? Cardiovascular risk in CKD? Urine protein versus albumin to creatinine Role of salt intake in CKD progression R2ID Protocol • 2300 patients with CKD stage 3 • Comprehensive clinical assessment – – – – – – Medical and Social History Sodium intake questionnaire Anthropomorphic measurements Blood and urine biochemistry (urine ACR and PCR) Skin AGE levels Arterial pulsewave velocity • Feedback letter to GP 2 R ID Protocol • Repeat clinical assessment at 1 year • Collect data regarding outcomes at year 2, 5 and 10: – – – – Change in GFR ESRD Cardiovascular events Death (via Med Research Info Service)























































![CKD talk[1].15.09 - Jacobi Medical Center](http://s1.studyres.com/store/data/003340080_1-9b582fb6e77d5fad41f81c427bfa5f30-150x150.png)