Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
INTRODUCTION TO
ICH Q8 & Q9 GUIDELINES
K. S. BABU
Head - Corporate Regulatory Affairs
Watson Pharma., India
November 29, 2007
FOREWORD
EMPHASIS
Interpretation of guidance documents
Regulatory relevance & applications
Bonus: Q10 guideline, due to its relevance
2
WHAT ARE THESE GUIDELINES ABOUT?
Q8:
- “Pharmaceutical Development” (“Implemented”)
- Contents of 3.2.P.2 Section of Module 3, CTD
Q8 – Annexure (“Draft stage”)
- Provides further clarification to Q8 concepts
- Links ‘’QbD’’ & “PAT” (FDA), & ‘’QRM’’ (EU), “FEMA”
Q9:
- “Quality Risk Management” (“Implemented”)
Q10: - “Pharmaceutical Quality System” (“Draft stage”)
3
REGULATORY STATUS OF ICH Q 8
Reached Step 5 – Regulatory Implementation
EU:
Transmission to CHMP and to Interested Parties in December 2004.
Issued as EMEA/CHMP/167068/2004-ICH. Deadline for comments :
June 2005. Final approval by CHMP: November 2005. Date for coming
into operation: May 2006.
MHLW:
Adopted on September 1, 2006, PFSB/ELD Notification N° 0901001
FDA:
Published in the Federal Register, Vol. 71, No 98, May 22, 2006
4
REGULATORY STATUS OF ICH Q 8 - Annexure
Reached Step 3 in Nov. 2007:
- Regulatory Consultation & Discussion
- Draft Guideline
EU / MHLW / FDA: TO BE NOTIFIED
5
REGULATORY STATUS OF ICH Q 9
Reached Step 5 – Regulatory Implementation
EU:
Published on the EMEA website
MHLW:
Adopted on September 1, 2006, PFSB/ELD Notification n°
0901004
FDA:
Published in the Federal Register, Vol. 71, No 106, pages
32105-32106, June 2, 2006
6
REGULATORY STATUS OF ICH Q 10
Reached Step 3 in May 2007:
- Regulatory Consultation & Discussion
- Draft Guideline
EU:
Transmission to CHMP and to Interested Parties May 2007. Issued as
EMEA/CHMP/ICH/214732/2007. Deadline for comments: November 2007.
MHLW:
Released for consultation 13th July 2007, PFSB/ELD, deadline for comments
1st October 2007
FDA:
Published in the Federal Register July 13, 2007, Volume 72, No. 134, pages
38604-38605. Deadline for comments October 11, 2007.
7
BRIEF NOTE ON ICH Q10 : P.Q.S.
• Based on ISO concepts
• Includes applicable GMP regulations
• Compliments ICH Q8 and ICH Q9
• Acts as a model for a pharmaceutical quality system that can be
implemented throughout the different stages of a product
lifecycle.
• Content is currently specified by regional GMP requirements
• Not intended to create any new expectations beyond current
regulatory requirements
• Consequently, the content of ICH Q10 that is additional to
current GMP requirements is optional
8
Q8: OVERVIEW
Talks about Pharmaceutical Dev. section in regulatory submissions
Suggested Contents for 3.2.P.2 of CTD Quality Module 3:
3.2.P.2.1 Components of drug product (drug substance/ excipients)
3.2.P.2.2 Formulation Dev.
3.2.P.2.3 Manufacturing Process Development
3.2.P.2.4 Container Closure System
3.2.P.2.5 Microbiological Attributes
3.2.P.2.6 Compatibility
There is “much more” than
meeting the filing requirements or CTD check-list
9
Q8: OVERVIEW (contd.)
Greater understanding of the product / process & variables
Science- and risk-based submissions
Wider regulatory “flexibility”
Q8 Annexure & “Q R M” (ICH Q9)
10
Q8: Related EU Directives and Guidelines
2003/63/EC, Annex I, 3.2.2.2 – Pharmaceutical Development
CPMP/QWP/155/96 Guideline on Development Pharmaceutics
NTA Volume 2B - Common Technical Document
Note for guidance on development pharmaceutics
(EMEA/CHMP/167068/2004)
Link to EU Directives:
http://ec.europa.eu/enterprise/pharmaceuticals/eudralex/homev1.htm
11
Q8: Objectives of Pharmaceutical Dev. Section
UNDERSTANDING: Provide a comprehensive understating of the product and
manufacturing process for reviewers and inspectors
EVIDENCE: Establish evidence that the dosage form, the formulation,
manufacturing process, container closure system, microbiological
attributes and usage instructions are appropriate for the intended use
ASSURANCE: Provide scientific discussion to support that –
the design / process will consistently deliver a quality product
SYSTEMATIC ASSESSMENT:
Testing during developmental stage – Extensive & Different from routine
Critical parameters of the formulation and process which can
influence batch reproducibility, medicinal product performance
and medicinal product quality shall be identified and described.
12
Q8: IMPORTANT CONSIDERATIONS
3.2.P.2.1.1 Drug Substance:
- Key physicochemical characteristics of the drug substance
(e.g. solubility, water content, particle size distribution), which are
variable and critical for the quality of the product and which can
influence the performance of the drug product
- Compatibility of drug substance with the excipients
- For combination products, the compatibility of the drug
substances with each other
- Polymorphism issues
13
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.1.2 Excipients:
- Choice of excipients (in particular relative to their respective
functions) & their concentration (with justification)
- Their characteristics that may influence the drug product
performance
- Compatibility of excipients with other excipients, where relevant
- Justification for their inclusion, in some cases (e.g.
preservatives, anti-oxidants) accompanied by experimental data
- Safety of the excipients, where relevant
14
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.2.1 Formulation Development:
- Differences between clinical formulations and current
formulation
- Summary describing the development of the formulation
including identification of critical attributes to the quality of the
drug product
- The choice of drug product components (drug substance,
excipients, container closure system etc.,) and the
manufacturing process
- Results of comparative in vitro studies (dissolution) and in vivo
studies (bio-equivalence), when appropriate
- Any special design features of the drug product (tablet score
line,over fill etc.,)
15
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.2.2 Overages:
- Use of an overage of a drug substance to compensate for
degradation during manufacture or a product’s shelf life, or
to extend shelf life, is discouraged
- A justification of any overage on grounds of safety and
efficacy
- Information on amount of overage, reason for the overage
and the justification for the amount of overage.
16
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.2.3 Physicochemical and Biological parameters:
- The physicochemical and biological properties
relevant to the safety, performance or
manufacturability of the drug product should be
identified and discussed
- The selection of dissolution testing should be
discussed.
17
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.3 – Manufacturing Process Development
- Basis for process improvement, process validation,
continuous process verification and process control
requirements.
- The selection, the control, and any improvement of
the manufacturing process.
- Appropriateness of the equipment used for the
intended product.
- For the sterile products, appropriate method of
sterilization and the primary packaging material
selection should be discussed.
18
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.3 – Manufacturing Process Development (contd.)
- Significant difference between the manufacturing process of
pivotal batches and intended commercial batches.
- If differences are there, the influence of the difference on
product performance, manufacturability and quality to be
discussed.
- Experiments of laboratory scale batches should be described.
- Information from scaling up from laboratory through pilot
to production scale to justify that scale-up can be achieved
without a consequent loss in quality.
19
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.4 – Container Closure System
- Discussion on the suitability of the container closure system
used for storage, transportation and use of the product
- This discussion should consider
•
•
•
•
choice of the materials for primary packaging
protection from moisture and light
compatibility of the materials with the dosage form
performance of the dose delivery from the device if
dosing device is used
• Food grade certification
20
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.5 – Microbiological Attributes
Where appropriate the microbiological attributes of the dosage form
should be addressed (according to Ph.Eur.). The discussion should
include for example:
• The rationale for performing or not performing microbial limits testing for
non-sterile products.
• The selection and effectiveness of preservative systems in products
containing antimicrobial preservatives.
• For sterile products, the integrity of the container closure system as it
relates to preventing microbial contamination.
The lowest concentration of antimicrobial preservative should be
demonstrated to be effective in controlling microorganisms.
21
Q8: IMPORTANT CONSIDERATIONS (contd.)
3.2.P.2.6 – Compatibility
• The compatibility of the drug product with
reconstitution diluent(s) should be addressed to
provide appropriate labelling information.
• This information should cover the recommended inuse shelf life at the recommended storage
temperature.
22
Q8: OVERVIEW (contd.)
Greater understanding of the product / process & variables
Science- and risk-based submissions
Wider regulatory “flexibility”
Q8 Annexure & “Q R M” (ICH Q9)
23
Specific Cases
• Use of one lot of API for Exhibit batches : PSD
Profile Optimization
• Impact of age of API used in Exhibit batches
• Blend time optimization
• Switching to alternate sources for Excipients
(E.g., Mg.Stearate– Animal grade to Veg. grade)
24
Focus of Q8 Annexure
•
•
•
•
•
Define Target Product Profile
Identify ‘CQAs’ – Critical Quality Attributes of Product
Determine QAs of inputs – materials/parameters etc.
Select appropriate process
Determine functional relationships between material
attributes & process parameters to Product CQAs
• Identify a control strategy
• Propose a “design space”
• Define and describe design space in regulatory
submission
25
Focus of Q8 Annexure (contd.)
Defining DESIGN SPACE: Options • Ranges of input variables or parameters
• Analysis of historical data can be basis
• Scaling factors
• Multivariate operations
Operation within the design space results in a product
that meets the defined quality attributes
Periodic reassessment throughout life-cycle
26
ICH Q 9 (QRM) as part of development
• To design a quality product and its manufacturing
process
- to consistently deliver the intended performance
of the product
• To enhance knowledge of product performance
over a wide range of
- material attributes
(e.g. particle size distribution, moisture content, flow
properties)
- processing options
- process parameters
27
QRM as part of development (contd.)
• To assess the critical attributes of
- Raw materials
- Solvents
- Active Pharmaceutical Ingredient (API)
- Starting materials
- Excipients
- Packaging materials
• To establish appropriate specifications, identify
critical process parameters and establish
manufacturing controls
28
QRM as part of development (contd.)
• To decrease variability of quality attributes:
- reduce product and material defects
- reduce manufacturing defects
• To assess the need for additional studies
(e.g., bioequivalence, stability)
relating to scale up and technology transfer
• To make use of the “design space” concept (annexure to
ICH Q8)
29
Q9 : QUALITY RISK MANAGEMENT
What is “risk”?
Combination of the probability of occurrence of
harm, and the severity of that harm.
“Fact: No process is risk-free”
30
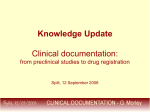
MANAGING RISKS IN A COMPANY …
Company
Strategic risks
Operational risks
Financial risks
Compliance risks
Environmental
Regulatory filing
Competitor
advantage
Company
viability
Shareholder
harm
Patient
harm
Quality / GMP
Safety & Efficacy
ICH Q9
31
EMEA NOTE ON Q9
32
Q9: Dangers from Absence of Risk Management
- Pharmaceutical products may not be available to patients when
needed, e.g. when a product is recalled from a market or where
different risk decisions contribute to inefficient manufacturing processes
and consequent delays
- May increase the potential for the release of unacceptable product to the
market
- Delays may occur during implementation of changes and improvements
to processes
- Safe and effective drugs may be discarded or recalled from the market
- Manufacturers may be reluctant to implement new technologies or
continuous improvements to products or processes
- Scarce resources may not be optimally allocated
- Lack of appropriate date to evaluate risk most effectively
33
Q9: Purpose & Objectives
• No national guidance documents in this area in any region
• No common understanding of terms, principles and application of risk
management
• Development of a harmonised pharmaceutical quality system applicable
across the life cycle of the product emphasising an integrated approach to
risk management and science
• Deriving common terminology, including a definition of quality, risk,
risk management etc
• Defining the principles for how risk management can be effectively applied
and consistently integrated into decisions regarding product quality
• Rationalization & Operationalization of the integration of risk
management into the decision making process
34
Q9: Purpose & Objectives (contd.)
• Defining criteria on how to apply the risk management process
• Identification of circumstances, if any, when applying risk management
principles is not feasible or appropriate
• Defining what principles of risk management apply to industry, regulators
or both across the life-cycle of the product
• Establish - how, what & when information is exchanged between & within
industry, to the regulators, and to both, throughout the product life cycle
• Emphasize synergies with the pharmaceutical development project
• Defining roles and responsibilities of regulators and industry
• Discuss how risk can be incorporated into resource allocation decisions
35
Q9: Benefits of Quality Risk Management Approach
• Enhancement of patient confidence worldwide in decision making on the
quality of pharmaceuticals
• Promotion of more effective use of regulatory and industry resources
• Establishment of a systematic, well-informed and thorough method of
decision making which leads to greater transparency and predictability
• Increased knowledge of exposure to risk
• A greater assurance to regulators of a company’s ability to deal with
potential risks
• Fostering continuous improvement and quality by design generally leading
to enhanced product quality
• Enables right “decision making”
36
Quality Risk Management Process
37
Risk Assessment
3 Stages:
Risk identification: what are the hazards?
Risk analysis: risk associated with identified hazards
Risk evaluation: comparison of identified and analyzed
risk against a given risk criteria
3 fundamental questions:
What might go wrong?
What is the likelihood it will go wrong?: Probability
What are the consequences? : Severity
38
Risk Control
Decision making:
Risk reduction? Or
Risk acceptance?
Basis for Judgment:
Is the risk above an acceptable level?
What can done to reduce or eliminate risks?
What is the appropriate balance among benefits, risks
and resources?
Are new risks introduced as a result of the identified risks
being controlled?
39
Risk Management methodology
Recognized risk management tools:
Basic risk management facilitation methods (Flow charts, check
sheets etc.).
Failure Mode Effects Analysis (FMEA).
Failure Mode, Effects and Criticality Analysis (FMECA).
Fault Tree Analysis (FTA).
Hazard Analysis and Critical Control Points (HACCP).
Hazard Operability Analysis (HAZOP).
Preliminary Hazard Analysis (PHA).
Risk Ranking and Filtering.
Supporting Statistical Tools.
40
Importance of Communication in QRM
Communication
facilitates trust
and understanding
Regulators
operation
Industry
operation
- Reviews
- Inspections
- Submissions
- Manufacturing
41
Using ICH Q9 will…
• Facilitate
- Communication and transparency
- More informed, scientifically based decision making
- Patient focused actions on quality risks
- Realistic and appropriate solutions
- Use of existing solutions (Share best practice/prior knowledge)
• Manage critical to quality aspects
- Through systems, organisations, processes & products
- Maintain responsibility & accountability for QRM
• Focus activity towards patient protection
It should never be used as a “hobby horse” / preconceived idea
42
Opportunity for the Industry & Competent Authorities
• Using the same guideline apply QRM to
industry (Development & Manufacture) and
regulators (Reviewer & Inspectorate)
• Provides for establishing a defined program
for what we already do every day in our jobs
• Supports science-based decision making
• Optimisation of resources
• Prevention from overly restrictive and
unnecessary requirements
• Facilitates communication and transparency
43
Challenges for Industry & Competent Authorities
• Interpreting and adopting the concepts
of quality risk management into specific areas
- Embed this behavior into quality aspects
of business, technology and regulation
- Adopt in existing structures, organizations
and Quality System
- Balance the documented use of “informal”
and “formal” quality risk management
44
QRM Integration into Industry & Reg Operations
QRM is a process that supports science-based and
practical decisions when integrated into quality systems.
Effective QRM can facilitate better and more informed
decisions.
Effective QRM can provide regulators with greater
assurance of a company’s ability to deal with
potential risks.
QRM can facilitate better use of resources by all
parties.
Training of both industry and regulatory personnel in
QRM processes provides for greater understanding of
decision-making processes & builds confidence in QRM
outcomes.
45
The new paradigm
“risk-based”
concepts and
principles
46
Incremental steps
Pharmaceutical Development (Q8)
Changed
Paradigm
Past:
Data transfer / Variable output
Present: Knowledge transfer / Science
based / Consistent output
Quality Risk Management (Q9)
Past:
Used, however poorly defined
Present: Opportunity to use structured
process thinking
Pharmaceutical Quality Systems (Q10)
Q9
Past:
GMP checklist
Future: Quality Systems across product
life cycle
47
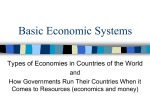
Low
en
t
m
pr
ov
e
im
co
nt
in
ua
l
High
Q10 Pharm. Quality Systems
Risk from Manufacturing site
How Q9 interacts with Q8 and Q10
Q8 Pharmaceutical Development
Low
Using Q9
Quality Risk
Management
principles
High
Product / Process Risk
48
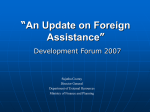
ICH Q9 Link back to patient risk
Opportunities to impact
risk using quality risk
management Q9
Design
Process
Materials
Facilities
Manufacturing
Distribution
Patient
Q8
Q10
49
A Vision of the Future
Old Approach
Broad Concept
Quality
Systems
Regulatory
New Approach
Remarks
Quality decisions divorced
from science and risk
evaluation.
Adherence to filing
commitments.
Quality decisions and filing
committments based
on Process
Understanding and
Risk Management.
Quality by Design.
Design Space concept
introduced to integrate
process knowledge with
regulatory evaluation.
Post-factum sampling and
quality testing.
Process Validation.
Management of variability
Process control
focused on critical
attributes.
Continuous Quality
Verification.
Quality by design definition
applied. Measure critical
process parameters to
control output product
quality.
Systems designed to inhibit
changes & minimize
business risks.
Discourages
improvement &
innovation.
Changes managed within
company's quality
system.
Real time batch
release feasible.
Regulators and industry
place higher reliance /
trust / understanding
on systems.
Multidisciplinary
evaluation and decision
making.
Compliance focus.
Changes require prior
approval.
Regulatory scrutiny adjusted
to level of Process
Understanding.
Continuous
improvement allowed
within Design Space.
Requires mechanisms to
communicate Process
Understanding data
("inspectable rather than
reviewable").
50
Regulatory Guidelines
Read… Repeat… Ruminate…
“raison d'être” (French; underlying principle)
THANK YOU !
51