Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
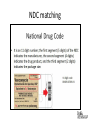
7th Annual GHA Compliance Officers Retreat September 3 – 5, 2014 Reynolds Plantation Greensboro, Georgia 340B Participation? What is your role? 10 MINUTE QUICK TOUR Program intent To permit covered entities “to stretch scarce Federal resources as far as possible, reaching more eligible patients and providing more comprehensive services.” H.R. Rep. No. 102-384(II), at 12 (1992) What is the 340B Drug Program? • Section 340B of the Public Health Service Act requires drug manufacturers who wished to sell drugs to the Medicaid program to provide reduced pricing. What is the 340B Drug Program? • Reduced pricing applies only to – covered entities, – covered patients, and – covered outpatient drugs. What is a covered entity? • Facilities or programs listed in the 340B Statute as eligible to purchase drugs through the 340B Program and appear on the Office of Pharmacy Affairs Database (OPA). – A pharmacy is not an eligible 340B covered entity. Which entities can participate? • Hospitals – Disproportionate Share Hospitals – Children’s Hospitals – Freestanding Cancer Hospitals – Rural Referral Centers – Sole Community Hospitals – Critical Access Hospitals • Community Health Centers/FQHCs • Certain specialized clinics (STD, HIV, etc.) Hospital DSH percentage? • Certain hospitals must meet disproportionate share adjustment percentages for the most recent cost reporting period before the calendar quarter involved: – Disproportionate Share, Children’s, Free Standing Cancer: > 11.75% – Sole Community, Rural Referral Center: ≥ 8% – CAH – no DSH requirement Additional requirements? • Additional requirements for hospitals – Must be owned and operated by state or local government, or – Private, non-profit under contract with state to provide care to indigent populations, or – Be granted governmental powers • Formal recognition to provide healthcare for medically indigent population in state What is a covered entity? • Facilities or programs listed in the 340B Statute as eligible to purchase drugs through the 340B Program and appear on the Office of Pharmacy Affairs Database (OPA). – A pharmacy is not an eligible 340B covered entity. OPA database Compliance look-out • Inaccurate OPA database information – 26% of 2013 HRSA audits – 29% of 2012 HRSA audits – Addresses, contacts, terminated covered entities, contract pharmacies How can this happen? What is a covered drug? • An FDA-approved prescription drug, an overthe-counter (OTC) drug that is written on a prescription, a biological product that can be dispensed only by a prescription (other than a vaccine), or FDA-approved insulin • Drugs can only be dispensed to qualifying outpatients. Compliance look-out How can this happen? 1996 definition Compliance look-out How can this happen? Compliance look-out • Ineligible patient • Ineligible prescriber Referrals? Are employees 340B eligible? GPO Prohibition • Applies to DSH, PEDs and CANs • Does not apply to CAHs, SCHs, RRCs Why a GPO prohibition? • Manufacturers feel that if a hospital is getting the 340B deep discount on covered outpatient drugs, it should not be entitled to additional GPO discounts for covered outpatient drugs. 34OB and GPO Compliance look-out • Which areas in the hospital system use drugs purchased under GPO contracts? – Inpatient only areas – Non-provider-based areas outside of four walls – Inside four walls ONLY if not legally part of the covered entity GPO tracking requirements Manual inventories • Prospective purchase methodology – Drugs purchased at the 340B discount price will kept physically separate from all other drugs – Drugs will be taken from the 340B manual inventory when needed to dispense to an eligible patient – Beginning and ending inventory counts should be reconciled considering purchases and eligible patient usage Manual inventories Purchase drugs at 340B prices GPO ? Chart/track use of drug Issue drug to eligible patient Maintain in a physically separate inventory Audit requirements Beginning Inventory Purchases Dispensations Returns/Adjustments Ending Inventory Compliance look-out • Do any of the 340B entities maintain manual inventories? • Can they be reconciled from purchase to dispense/administration to a patient? Virtual inventories • Replenishment methodology – Drugs purchased at 340B discount can be commingled with other drugs – Drugs will be dispensed to patient, and dependent upon patient type, will be tracked as a 340B dispense (use tracking software) – 340B dispensations will be used to support future 340B purchases Tracking dispensations for support Dispensations or claims feed Drug purchasing audit trail 340B Must have supporting dispensations to support orders Must have supporting dispensations to support orders GPO Compliance look-out • Are dispensations in 340B tracking software (GPO and 340B) tested routinely for: – Drug conversion accuracy – Dosage compared to medical chart – Location of patient at time of dispense – Posting of ALL purchases – NDC matching NDC matching NDC tracking requirements • Drugs purchased to replace stock used on 340B eligible patients must bear the same National Drug Code (NDC) 11-digit match as the one dispensed. • Exceptions are very limited and can be replenished only in cases where only a 9 digit match is available. • This NDC-to-NDC match is difficult and sometimes impossible to achieve. Multiple NDCs How do I know which NDC was given to patient? Since we don’t use bar codes, I will have to use one NDC as the proxy. Drug – ABC is purchased using two NDCs. • NDC 1 • NDC 2 2 2 1 2 1 1 2 Primary NDC Primary NDC – most common 340B purchase Less common versions of same drug Secondary NDC A Secondary NDC B Secondary NDC C Dispensations flow to accumulator with this NDC for 340B replenishment Actual NDCs will not flow to accumulator until designated as the primary. Cannot be replenished under 340B until shows up in accumulator. Compliance look-out • How often are primary NDCs revised? – Dispense “feed” to accumulator – Charge “feed” to accumulator • Are only “exact” 11-digit matches used in replenishment, or are “substitutions” used? • How often are 340B/GPO replenishments tested for support? Compliance look-out There are savings up to 50% on drug costs. WHAT’S THE FUSS? • Volume of 340B purchases • Use of contract pharmacies • Public comments regarding 340B participation • Prior history 340B 340B avg. annual savings - $31.7 million Contract pharmacies • Are contract pharmacy arrangements profitable? Summary • • • • Understand the compliance risks Participate in monitoring and audits Educate yourself and staff Keep a look-out for Program changes For more information Cindy DuPree, CPA [email protected] 404.220.8494 Sarah Dekutowski, CPA [email protected] 404.220.8494