Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
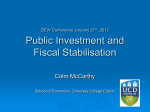
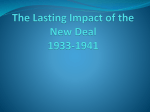
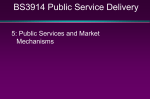
Budget Analysis for Expenditure Rationalization Public Finance Analysis and Management Course World Bank, April 23-27, 2007 Marijn Verhoeven Expenditure Policy Division Fiscal Affairs Department, IMF Overview • Why expenditure rationalization? • The analytical tool box for expenditure rationalization: – A word about data – Measuring efficiency • We found the problems—now what? (very briefly!) Why expenditure rationalization? • To achieve macroeconomic stability and fiscal sustainability • To create fiscal space • To increase allocative efficiency by cutting back or reforming government activities • To enhance X-efficiency by achieving the same outputs with less inputs Why expenditure rationalization? (cont’d) Figure 5: Fiscal Space Increase of Grant Aid in % GDP 5 4 3 2 Improved Expend. Efficiency in % GDP 1 0 New Borrowing in % GDP Improved Revenue Effort in % GDP A word about data • Expenditure analysis is typically data driven • But data are problematic • There are several competing sources of spending data, each with their strengths and weaknesses • Let us look at the example of data on wage spending Facts and figures: measuring wage spending • The wage bill is measured: – As a share of GDP and total spending to compare across countries – As a share of domestic revenue to assess sustainability – At the sectoral level, compare to nonwage spending to assess efficiency • Source is IMF Government Finance Statistics or national data Table 1. Central Government Wages and Salaries, 1990-2001 Sample Size Central government wages and salaries in percent of GDP Central government wages and salaries in percent of central government expenditure Africa Francophone Africa Non-Francophone Africa Asia South Asia 11 6 5 10 3 8.4 6.3 10.9 5.3 4.6 28.3 27.7 29.0 20.0 15.1 Europe and Central Asia Central and Eastern Europe Latin America & the Caribbean Caribbean countries Middle East and North Africa 21 12 16 3 6 3.9 5.1 5.6 8.6 9.1 12.6 14.4 25.0 31.1 30.4 European Union 15 5.4 13.3 Low-Income Countries Middle-Income Countries High-Income Countries 19 42 30 5.7 6.0 5.9 22.6 22.1 15.6 Memorandum items: PRGF-Supported Programs 1/ OECD General Government 2/ 28 21 4.8 11.4 19.9 Country Group Sources: Government Financial Statistics database (IMF); International Financial Statistics database (IMF); World Economic Outlook database (IMF); and IMF Staff. 1/ Data refers to 2001 outturn. 2/ OECD, 2000, "Summary of the Public Sector Pay and Employment Data Analysis and Future Direction for HRM Data Collection." Data refers to 1997 total compensation cost, which includes the wage bill and employer contributions to social insurance. Lies and statistics: mismeasuring wage spending? • Not all compensation may be captured in wages and salaries: transfers (pension benefits and subventions for education), other goods and services (in-kind benefits and contractual workers), and capital spending (donor-financed projects) may hide substantial wage spending. In Nicaragua, out of actual wage spending of 8.6 percent in 2005, less than 4 percent is recorded as wages and salaries. • When government is decentralized, central government wage spending is biased downward. But reliable data for general government are rare for low-income countries. Efficiency: the issue Source: World Bank (2004) World Development Report 2004. Spending refers to total annual public spending per child of primary school age, in 1995 US dollars. How should we think about the efficiency of public spending? • What is the mix of public programs that best meets government objectives? – Where to invest the marginal dollar across sectors • For example, can education goals be reached by investing the marginal dollar in other sectors? – Where to invest the marginal dollar within sectors • Primary versus secondary education • Primary health care versus secondary health care How should we think about the efficiency of public spending? (cont’d) • Given allocative decisions, is output maximized with given inputs? – Common problems: • Inappropriate student/teacher ratios • Shortage of medicine or nurses relative to doctors • Shortage of textbooks • Waste, leakage of funds • Labor and utility costs crowding out maintenance and capital spending Assessing efficiency Many roads lead to Rome: • “Basic” benchmarking • PETS • Randomized evaluations • Absenteeism studies • Sectoral efficiency analysis Choice depends on data availability, objectives, and priors Assessing efficiency always begins with... Review the basics of public spending • Functional classification – Primary, secondary, tertiary education • Inputs, programs, types of intervention – Education: Teachers, textbooks – Health: Spraying, information and education campaign, etc. • Economic classification – Wage versus non-wage – Recurrent versus capital (investment) spending • Central and local government budgets, other Ministries • Planned versus actual, nominal versus real • Share of private, NGO, and donor spending “Basic” benchmarking • Selected useful descriptive statistics – Budget data – Unit costs – Ratios of teachers, students, non-teaching staff – Distribution of teachers among levels of qualifications; percentage meeting basic government standards – Actual maintenance budget versus engineering estimates for routine maintenance – Enrollment rates, repetition rates, dropout rates – Absenteeism, informal payments, etc. “Basic” benchmarking (cont’d) • Comparisons – Sub-national units, clinics, schools – Private versus public schools – Private versus public health facilities – Comparator countries • Cross-country information on real resources and output – UNESCO education indicators – Program for International Student Assessment (PISA) – WHO Indicators of Health System Attainment – Trends in International Mathematics and Science Study (TIMSS) – Progress in International Reading Literacy Study (PIRLS) and the International Survey of Adults (ISA) Randomized evaluations Randomized evaluations of educational reform programs: • Random selection of schools for the reform – Colombian voucher program, Angrist and others (2002) • Randomized phase-in of programs – Argentina: Decentralization took place across all provinces, but at different periods and intensities, Galliani and Schargrodsky (2002) Public expenditure tracking surveys Trace the flow of resources through the bureaucracy from the central government down to the service facility: • Comparing originally allocated funds with funds that actually arrive at the facility • Amount of time required for fund to arrive • Reinikka and Svensson (2001): Uganda in the 1990s, significant leakage existed Sectoral efficiency analysis: basic concepts • The measurement of efficiency generally requires the following: – (i) information on inputs and associated costs; – (ii) an estimation of output or benefit; and – (iii) a comparison of (i) and (ii) • Key question: – Could the same level of output be achieved with less input? – Equivalently, could more output be generated with the same level of input? Sectoral efficiency analysis: basic concepts (cont’d) Overall efficiency Health Expenditure Public health expenditure Private health expenditure Cost effectiveness Real Health Resources (examples) Hospital beds Physicians/health workers Immunizations Doctors’ consultations In-patient admissions Lengths of stay Bed occupancy rate Health Outcomes Health adjusted life expectancy Standardized death rate Infant mortality rate Child mortality rate Maternal mortality rate Incidence of tuberculosis System efficiency Sectoral efficiency analysis: Best-practice frontier 3 2.5 Product item F C B 2 1.5 D A 1 E 0.5 0 0 0.2 0.4 0.6 0.8 Input item 1 1.2 1.4 Sectoral efficiency analysis: measuring efficiency • Basic idea: measuring distance from the bestpractice frontier • Regression analysis – Corrected ordinary least squares (COLS) • Evans et al (2000), WHO (2000): Efficiency of national health systems – Alternative: Greene (2004): Stochastic frontier analysis • Nonparametric analysis: – Free disposal hull analysis (FDH) • Gupta and Verhoeven (2004) (Chapter 11): Efficiency of health and education spending in 85 countries, 1984-95 – Data envelopment analysis (DEA) • Herrera and Pang (2005): Efficiency of health and education spending in 140 countries, 1996-2002 • Affonso and St. Aubyn (2004): Efficiency of health and education spending in OECD countries Sectoral efficiency analysis: problems • Lack of insight in nature of relationship between inputs and outputs: – – – – How to measure inputs and outputs? Lags? Impact of environmental factors? Externalities across sectors? • Parametric approaches are very data intensive and require more assumptions about the relationship • Nonparametric approaches are less robust (e.g., small sample bias) and sensitive to outliers • The analysis is only as good as the data—and data are weak (e.g., on quality and policy objectives) Examples of FAD sectoral efficiency analysis • FAD research: – The efficiency of education, health, and social assistance spending in EU New Member States – The efficiency of education and health spending in the G7 – The efficiency of government investment in Latin America • Focus here on the efficiency of health spending in the Slovak Republic Output-Oriented Efficiency Relative to the OECD (distribution by quartiles of the ranking of OECD bias-corrected output-oriented efficiency scores) 1/ Percentile Public expenditures Public and private expenditures 1-25 Bulgaria 26-50 Czech Republic Latvia Bulgaria Czech Republic Slovak Republic Estonia Romania Poland 51-75 Estonia Poland Slovak Republic Slovenia Lithuania Slovenia 76-100 Hungary Lithuania Romania Hungary Latvia Source: IMF staff calculations 1/ Slovak Republic’s output-oriented efficiency scores for public expenditures ranked, on average, at the 54th percentile of the overall ranking of efficiency scores in the sample of OECD countries. This places Slovak Republic in the third (51-75) quartile of the OECD ranking distribution. The rankings are based on each country’s average of the individual point estimates of the bias-corrected output-oriented efficiency scores for various outcome indicators, including infant, child, and maternal mortality, the incidence of tuberculosis and HALE (see Appendix II). Rank of Health Efficiency Scores Relative to the OECD 1/ Slovak Republic Bulgaria Czech Republic Estonia Hungary Latvia Lithuania Poland Romania Slovenia System Efficiency 2/ Intermediate Resources to outcomes 1.7 2.0 1.4 1.9 1.9 2.2 2.0 1.6 2.0 0.7 NMS-10 average EU-15 average 1.7 0.9 Overall Efficiency 3/ Public and private expenditures to Public expenditures to outcomes outcomes 1.1 0.4 0.5 0.5 0.7 0.5 1.4 0.7 1.5 1.4 1.0 1.5 1.6 1.1 1.0 0.5 1.5 0.6 1.1 1.0 1.1 1.0 0.8 1.1 Source: IMF staff calculations 1/ Ratio of output-oriented efficiency rankings of NMS-10 and EU-15 countries and the average ranking in the sample of OECD countries. The ratio is 1 if the country is as efficient as the average for the OECD, and is higher if the country is less efficient (see Appendix II). 2/ Based on output-oriented efficiency rankings using as inputs the average ranking of various real resources (Table 3) and as output various outcome indicators, including infant, child, and maternal mortality, the incidence of tuberculosis and HALE. 3/ Reflecting the output-oriented efficiency rankings of Table 6. SVK health efficiency: sources of inefficiencies • Low co-payments • Unproductive spending on administration and collective care • High spending on pharmaceuticals • High doctors’ consultations, outpatient contacts, and inpatient hospital care Key challenge is changing the mix of real resources! SVK health efficiency: recommendations • Restrain pharmaceutical spending – introducing a national procurement system – introducing incentives for generics – improving the pharmaceutical pricing and reimbursement policy of the Ministry of Health • Reduce the reliance on hospitals and contain the cost of hospital care – Eliminate excess hospital beds – Impose hard budget constraint on public hospitals – Restart hospital privatization • Reintroduce co-payments for doctors’ visits and hospital care SVK health efficiency: recommendations (cont’d) • Enhance incentives for competition and more cost-effective administrative arrangements – Introduce incentives for practitioners to be cost-effective – Define a stricter basic health care package, thereby allowing some variations in basic insurance premiums – Increase the power of the Antitrust authority and enhance the autonomy and independence of the Health Care Supervisory Board – Refrain from introducing new limitations on profits of private insurance companies Thank You!