Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
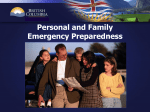
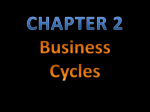
Manitoba Department of Finance Presentation to the Commission on the Future of Health Care in Canada Greg Selinger Minister of Finance Winnipeg - March 6, 2002 Overview • Sustainability of health care must be considered in the context of the Canadian federation itself and the fiscal arrangements that underpin it • The fiscal imbalance existing between the two orders of government is addressed mainly through the CHST mechanism • Sustainability of health and other programs hinges on achieving an effective balance Spending/Financing Developments • Health care’s share of provincial budgets increased over the 1990s • Key factors: – provincial decision to reinvest in Health Care in response to public concerns that access and quality was deteriorating – federal cuts in CHST - crowding out other areas Net Change in Program Spending by Source of Funding, 1994/95 to 1997/98 ($ billions) 5 Change in Provincial Own-Source Spending 4 Change in Federal CHST cash Funding Net Change in Spending 3 2 1 0 -1 -2 -3 -4 Health Care Other Programs Crowding-Out • Health Care demands have been met at the expense of other needs -- education, justice, social services, infrastructure and economic development • Not a viable long-term solution since these form the base upon which we maintain and afford our health care system Health as a Share of Manitoba's Budget, Baseline Projection to 2020/21 55% 50% 45% 40% 35% 30% 1990/91 1995/96 2000/01 2005/06 2010/11 2015/16 2020/21 Not just a Long-term Issue • Sustainability has a more immediate dimension • Provinces are facing a large and immediate cash crunch as well as difficult choices, while … • The December Fiscal Monitor points to $10 b surplus for the federal government in 2001/02 • Health as a percentage of GDP is expected to set new high water marks over the medium term Health Expenditure as a Percentage of GDP, by Component 12 Forecast Private Sector Other Public 10 Net Provincial Federal Cash 8 6 4 2 0 1981 1986 1991 1996 2001p 2006f CHST • Federal funding for provincial social programs has been eroded since the inception of EPF through a series of unilateral federal changes to the funding formula • CHST cash as a share of provincial social program funding averaged about 18% in the first half of the 1990’s, fell to 11% by 1998/99 • The current level of 14% is forecast to fall to 13% Federal Cash Transfers as a Share of Total Provincial/Territorial Government Spending on Major Social Programs 25% 20% 15% 10% 5% 0% 1985/86 1990/91 1995/96 2000/01 2005/06f CHST • Manitoba favours a durable CHST-based solution to the problem of funding health care • Options like the recent proliferation of federal “tiedfunding” schemes should be avoided since – ongoing provincial funding commitments are not matched by federal government, – they discriminate against provinces with lower fiscal capacity, and – they fail to reflect provincial priorities. CHST and Federalism • Need to adopt a more cooperative than unilateral model to restore confidence in partnership • Current CHST funding levels are arbitrary – not based on actual costs – not based on ability to pay (revenue capacity) – not based on a negotiated or agreed to “share” • Federal/provincial cooperation and decisionmaking to sustain CPP is a better model Conclusion • The task we face is not just to balance our own books, but to do it in a way that does not compromise our long-term economic potential and the provision of important public services • Our single-payer publicly administered health care system confers a cost advantage that must be preserved Conclusion • There is probably enough fiscal capacity in government - writ large - to manage the cost pressures over the next decade, if we plan well • The challenge is federal government needs to become more fully engaged in funding health care through the CHST to address both the immediate cost pressures and the larger ones that loom in the coming decades