Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
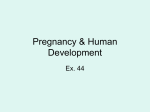
Lecture 12 Pregnancy and Human Development Figure 28.1 Diagrams showing the approximate size of a human conceptus from fertilization to the early fetal stage. Embryo Fertilization 1-week conceptus 3-week embryo (3 mm) 5-week embryo (10 mm) 8-week embryo (22 mm) 12-week fetus (90 mm) © 2013 Pearson Education, Inc. From Egg to Zygote • Sperm has a limited amount of time to reach the ovulated secondary oocyte • Oocyte is viable for 12 to 24 hours • Sperm viable 24 to 48 hours after ejaculation • Maximum likelihood of fertilization: coitus must occur no more than – Two days before ovulation – 24 hours after ovulation Fertilization • Sperm's chromosomes combine with those of secondary oocyte to form fertilized egg – zygote The Roadblocks • Most sperm don’t reach the oocyte • Ejaculated sperm – Leak out of vagina immediately after deposition – Destroyed by acidic vaginal environment – Fail to make it through cervix – Dispersed in uterine cavity or destroyed by phagocytes Capacitation • Fresh sperm are incapable of penetrating an oocyte – capacitated before they can penetrate oocyte – occurs 2 – 10 hrs after ejaculation – Sperm must become motile – Secretions of female tract weaken acrosome membrane • helps in the release of hydrolytic enzymes needed to penetrate oocyte • Calcium uptake to trigger motility Sperm can smell • Sperm have olfactory receptors that respond to chemical stimuli – presumed to be coming from the oocyte or surrounding area Sperm Penetration • Sperm must breach oocyte coverings – Corona radiata and zona pellucida • Corona radiata easier to get through • Zona pellucida requires an acrosomal reaction – Hyaluronidase, acrosin, proteases released to digest holes in zona pellucida ZP3 Glycoprotein • Zone pellucida receptor protein for sperm to bind • Binding opens a Ca2+ channel in sperm that activates the acrosomal reactions Plasma Membrane Fusion • Sperm head approaches oocyte – Rear portion of acrosomal membrane binds to oocyte plasma membrane • Binding has two consequences: – Oocyte forms microvilli that surround sperm and fuse membranes – Cytoplasmic contents of sperm enter the oocyte, leaving PM behind Figure 28.2 Sperm Penetration and the Cortical Reaction. 2 Acrosomal reaction. Binding of the sperm to sperm-binding receptors in the zona pellucida causes the Ca2+ levels within the sperm to rise, triggering the acrosomal reaction. Acrosomal enzymes from many sperm digest holes through the zona pellucida, clearing a path to the oocyte membrane. © 2013 Pearson Education, Inc. Zona pellucida Sperm-binding receptors Slide 3 Figure 28.2 Sperm Penetration and the Cortical Reaction. 3 Binding. The sperm’s membrane binds to the oocyte’s Sperm-binding receptors. © 2013 Pearson Education, Inc. Oocyte sperm-binding Membrane receptors Slide 4 Figure 28.2 Sperm Penetration and the Cortical Reaction. 4 Fusion. The sperm and oocyte plasma membranes fuse, allowing sperm contents to enter the oocyte. © 2013 Pearson Education, Inc. Cortical granules Slide 5 Monospermy • Upon entry of sperm, Ca2+ surge from ER causes cortical reaction: – Cortical granules release enzymes (zonal inhibiting proteins, or ZIPs) – ZIPs inactivate sperm receptors – Activates oocyte to prepare for second meiotic division Formation of the Zygote • Sperm nucleus moves toward oocyte nucleus and swells to form male pronucleus • Ovum nucleus swells to become female pronucleus • Fertilization – moment when membranes of two pronuclei rupture and chromosomes combine – zygote Figure 28.3b Events of fertilization. Male and female pronuclei Polar bodies © 2013 Pearson Education, Inc. Embryonic Development • Occurs while zygote moves toward uterus • Proccess called cleavage – rapid mitotic divisions without growth Cleavage • Mitotic divisions of zygote – First cleavage at 36 hours two daughter cells (blastomeres) – At 72 hours morula (16 or more cells) – At day 4 or 5, blastocyst (embryo of ~100 cells) reaches uterus The Blastocyst • Blastocyst - fluid-filled hollow sphere composed of: • Trophoblast cells – Display immunosuppressive factors – Participate in placenta formation • Inner cell mass – Becomes embryonic disc (embryo and three of embryonic membranes) Figure 28.4 Cleavage: From zygote to blastocyst. 4-cell stage 2 days Zygote (fertilized egg) Morula (a solid ball of blastomeres). 3 days Zona pellucida Degenerating zona pellucida Sperm Blastocyst cavity Uterine tube Fertilization (sperm meets and enters egg) Early blastocyst (Morula hollows out, fills with fluid, and “hatches” from the zona pellucida). 4 days Implanting blastocyst (Consists of a sphere of trophoblast cells and an eccentric cell cluster called the inner cell mass). 7 days Ovary Oocyte (egg) Trophoblast Ovulation Uterus Endometrium Cavity of uterus © 2013 Pearson Education, Inc. Blastocyst cavity Inner cell mass Implantation • Blastocyst floats for 2–3 days • Nourished by uterine secretions • Implantation begins 6–7 days after ovulation • Dependent on proper endometrial layer – minimum of 67% of all zygotes formed fail to implant – 30% of implanted zygotes miscarry due to varied factors Implantation • Trophoblasts proliferate and form two distinct layers – Cytotrophoblast (cellular trophoblast) - inner layer of cells – Syncytiotrophoblast (syncytial trophoblast) - cells in outer layer lose plasma membranes, invade and digest endometrium • Endometrial cells cover and seal off implanted blastocyst Figure 28.5a Implantation of the blastocyst. Endometrium Uterine endometrial epithelium Inner cell mass Trophoblast Blastocyst cavity Lumen of uterus © 2013 Pearson Education, Inc. Figure 28.5c Implantation of the blastocyst. Endometrial stroma with blood vessels and glands Syncytiotrophoblast Cytotrophoblast Blastocyst cavity Lumen of uterus © 2013 Pearson Education, Inc. Implantation • Implantation completed by twelfth day after ovulation – just before endometrium normally begins to slough off • Menstruation must be prevented • Viability of corpus luteum maintained by hormone human chorionic gonadotropin (hCG) Human chorionic gonadotropin (hCG) • Initially secreted by trophoblast cells – Prompts corpus luteum to continue secretion of progesterone and estrogen – Promotes placental development • hCG levels rise until end of second month, then decline as placenta begins to secrete progesterone and estrogen Figure 28.6 Hormonal changes during pregnancy. Relative blood levels Human chorionic gonadotropin Estrogens Progesterone 0 4 8 Ovulation and fertilization © 2013 Pearson Education, Inc. 12 16 24 20 28 Gestation (weeks) 32 36 Birth Placentation • Formation of placenta from embryonic and maternal tissues • Orginates from embryonic and endometrial tissues • Inner mass cells give rise to extraembryonic mesoderm layer – under the inner surface of trophoblast – This becomes the chorion Chorion and Chorionic villi • Chorion – outmost membrane that helps form the placenta – chorion grown outward to make chorionic villi – extending further into the endometrium layer that is growing new blood vessles • Maternal endometrium becomes the decidua basalis Placentation • Maternal portion of placenta – Decidua basalis – stratum functionalis between chorionic villi and stratum basalis of endometrium) • Fetal portion of placenta – Chorionic villi Figure 28.7a–c Events of placentation, early embryonic development, and extraembryonic membrane formation. Endometrium Lacuna (intervillous space) containing maternal blood Maternal blood vessels Proliferating syncytiotrophoblast Chorionic villus • Ectoderm Chorion • Mesoderm Amnion • Endoderm Cytotrophoblast Amniotic cavity Yolk sac Implanting 71/2 -day blastocyst. The syncytiotrophoblast is eroding the endometrium. Cells of the embryonic disc are now separated from the amnion by a fluid-filled space. © 2013 Pearson Education, Inc. Forming umbilical cord Allantois Bilayered embryonic disc • Epiblast • Hypoblast Endometrial epithelium Amniotic cavity Primary germ layers Extraembryonic mesoderm Chorion being formed Lumen of uterus 12-day blastocyst. Implantation is complete. Extraembryonic mesoderm is forming a discrete layer beneath the cytotrophoblast. Extraembryonic coelom 16-day embryo. Cytotrophoblast and associated mesoderm have become the chorion, and chorionic villi are elaborating. The embryo exhibits all three germ layers, a yolk sac, and an allantois, which forms the basis of the umbilical cord. Figure 28.7d Events of placentation, early embryonic development, and extraembryonic membrane formation. Decidua basalis Maternal blood Chorionic villus Umbilical blood vessels in umbilical cord Amnion Amniotic cavity Yolk sac Extraembryonic coelom Lumen of uterus Chorion Decidua capsularis 41/2 -week embryo. The decidua capsularis, decidua basalis, amnion, and yolk sac are well formed. The chorionic villi lie in blood-filled intervillous spaces within the endometrium. The embryo is nourished via the umbilical vessels that connect it (through the umbilical cord) to the placenta. © 2013 Pearson Education, Inc. Figure 28.7e Events of placentation, early embryonic development, and extraembryonic membrane formation. Placenta Decidua basalis Chorionic villi Yolk sac Amnion Amniotic cavity Umbilical cord Decidua capsularis Extraembryonic coelom 13-week fetus. © 2013 Pearson Education, Inc. Uterus Lumen of uterus Placentation • Placenta fully formed and functional by end of third month • Nutritive, respiratory, excretory, endocrine functions • Placenta also secretes human placental lactogen, human chorionic thyrotropin, hCG, and relaxin – inadequate hCG induces spontaneous abortion Placentation • Maternal and embryonic blood supplies normally do not intermix • Embryonic placental barriers include – Membranes of chorionic villi – Endothelium of embryonic capillaries Figure 28.8 Detailed anatomy of the vascular relationships in the mature decidua basalis. Placenta Chorionic villi Decidua basalis Maternal arteries Umbilical cord Decidua capsularis Uterus Lumen of uterus Chorionic villus containing fetal capillaries Maternal blood in lacuna (intervillous space) Fetal arteriole Fetal venule Amnion Umbilical cord © 2013 Pearson Education, Inc. Maternal veins Myometrium Stratum basalis of endometrium Maternal portion of placenta (decidua basalis) Fetal portion of placenta (chorion) Umbilical arteries Umbilical vein Connection to yolk sac Extraembryonic Membranes • Amnion – transparent sac filled with amniotic fluid – Provides buoyant environment that protects embryo – Helps maintain constant homeostatic temperature – Allows freedom of movement; isolates growing fetus – Amniotic fluid comes from maternal blood, and later, fetal urine Extraembryonic Membranes • Yolk sac - sac that hangs from ventral surface of embryo – Forms part of digestive tube – Source of earliest blood cells and blood vessels Extraembryonic Membranes • Allantois - small outpocketing at caudal end of yolk sac – Structural base for umbilical cord – Becomes part of urinary bladder Figure 28.7a–c Events of placentation, early embryonic development, and extraembryonic membrane formation. Endometrium Lacuna (intervillous space) containing maternal blood Maternal blood vessels Proliferating syncytiotrophoblast Chorionic villus • Ectoderm Chorion • Mesoderm Amnion • Endoderm Cytotrophoblast Amniotic cavity Yolk sac Implanting 71/2 -day blastocyst. The syncytiotrophoblast is eroding the endometrium. Cells of the embryonic disc are now separated from the amnion by a fluid-filled space. © 2013 Pearson Education, Inc. Forming umbilical cord Allantois Bilayered embryonic disc • Epiblast • Hypoblast Endometrial epithelium Amniotic cavity Primary germ layers Extraembryonic mesoderm Chorion being formed Lumen of uterus 12-day blastocyst. Implantation is complete. Extraembryonic mesoderm is forming a discrete layer beneath the cytotrophoblast. Extraembryonic coelom 16-day embryo. Cytotrophoblast and associated mesoderm have become the chorion, and chorionic villi are elaborating. The embryo exhibits all three germ layers, a yolk sac, and an allantois, which forms the basis of the umbilical cord. Figure 28.7d Events of placentation, early embryonic development, and extraembryonic membrane formation. Decidua basalis Maternal blood Chorionic villus Umbilical blood vessels in umbilical cord Amnion Amniotic cavity Yolk sac Extraembryonic coelom Lumen of uterus Chorion Decidua capsularis 41/2 -week embryo. The decidua capsularis, decidua basalis, amnion, and yolk sac are well formed. The chorionic villi lie in blood-filled intervillous spaces within the endometrium. The embryo is nourished via the umbilical vessels that connect it (through the umbilical cord) to the placenta. © 2013 Pearson Education, Inc. Gastrulation: From Gastrula to Fetus • While implanting is occuring, the blastocyst is being converted to a gastrula – three germ layers form – extraembroyonic membranes develop • To start: inner mass cells subdivide into two layers: – upper epiblast – lower hypoblast Figure 28.7a–c Events of placentation, early embryonic development, and extraembryonic membrane formation. Endometrium Lacuna (intervillous space) containing maternal blood Maternal blood vessels Proliferating syncytiotrophoblast Chorionic villus • Ectoderm Chorion • Mesoderm Amnion • Endoderm Cytotrophoblast Amniotic cavity Yolk sac Implanting 71/2 -day blastocyst. The syncytiotrophoblast is eroding the endometrium. Cells of the embryonic disc are now separated from the amnion by a fluid-filled space. © 2013 Pearson Education, Inc. Forming umbilical cord Allantois Bilayered embryonic disc • Epiblast • Hypoblast Endometrial epithelium Amniotic cavity Primary germ layers Extraembryonic mesoderm Chorion being formed Lumen of uterus 12-day blastocyst. Implantation is complete. Extraembryonic mesoderm is forming a discrete layer beneath the cytotrophoblast. Extraembryonic coelom 16-day embryo. Cytotrophoblast and associated mesoderm have become the chorion, and chorionic villi are elaborating. The embryo exhibits all three germ layers, a yolk sac, and an allantois, which forms the basis of the umbilical cord. Gastrulation • Occurs in week 3 • Embryonic disc forms three-layered embryo with primary germ layers: – Ectoderm, mesoderm, and endoderm • Begins with appearance of primitive streak – raised dorsal groove – establishes longitudinal axis of embryo Figure 28.9 Formation of the three primary germ layers. Amnion Bilayered embryonic disc Head end of bilayered embryonic disc Yolk sac Frontal section 3-D view Section view in (e) Primitive streak Head end Cut edge of amnion Epiblast Yolk sac (cut edge) Right Left 14-15 days Hypoblast Endoderm Ectoderm Primitive streak Tail end Bilayered embryonic disc, superior view © 2013 Pearson Education, Inc. 16 days Mesoderm Endoderm Organogenesis • Gastrulation sets stage for organogenesis – Formation of body organs and systems • At eighth week – All organ systems recognizable – End of embryonic period Ectoderm, mesoderm, endoderm • The primitive tissues from which all body organs derive • Ectoderm – “outer skin” – nervous system; skin epidermis • Endoderm – “inner skin” – epithelial linings of digestive, respiratory, urogenital systems; associated glands • Mesoderm – “middle skin” – everything else Organogenesis • Embryo begins as flat plate • Forms a cylindrical body resembling three stacked sheets of paper folding laterally into tube, and at both ends Figure 28.10a Folding of the embryonic body, lateral views. Head Tail Amnion Yolk sac Ectoderm Mesoderm Endoderm © 2013 Pearson Education, Inc. Trilaminar embryonic disc Figure 28.10b Folding of the embryonic body, lateral views. Lateral fold © 2013 Pearson Education, Inc. Future gut (digestive tube) Figure 28.10c Folding of the embryonic body, lateral views. Somites (seen through ectoderm) Tail fold Head fold Yolk sac © 2013 Pearson Education, Inc. Figure 28.10d Folding of the embryonic body, lateral views. Neural tube Notochord Primitive gut Hindgut © 2013 Pearson Education, Inc. Yolk sac Foregut Specialization of the Endoderm • Primitive Gut – becomes the epithelial lines of the GI tract – Organs of GI tract become apparent, and oral and anal openings perforate – Mucosal lining of respiratory tract forms from pharyngeal endoderm (foregut) – Glands arise further along tract Figure 28.11 Endodermal differentiation. Pharynx Parathyroid glands and thymus Thyroid gland Esophagus Trachea Connection to yolk sac Right and left lungs Stomach Liver Umbilical cord Pancreas Gallbladder Small intestine Allantois Large intestine © 2013 Pearson Education, Inc. 5-week embryo Specialization of the Ectoderm • Neurulation – First major event of organogenesis – Gives rise to brain and spinal cord – Induced by chemical signals from notochord – Ectoderm over notochord thickens, forming neural plate – Neural plate folds inward as neural groove with neural folds Specialization of the Mesoderm • First evidence - appearance of notochord – Eventually replaced by vertebral column • Formation of somites – mesodermal aggregates • Formation of Intermediate mesoderm • Formation of Lateral plate mesoderm Figure 28.12a Neurulation and early mesodermal differentiation. Head Amnion Amniotic cavity Left Right Cut edge of amnion Primitive streak Tail Neural plate Ectoderm Mesoderm Notochord Endoderm Yolk sac © 2013 Pearson Education, Inc. 17 days. The flat three-layered embryo has completed gastrulation. Notochord and neural plate are present. Figure 28.12b Neurulation and early mesodermal differentiation. Neural crest Neural groove Neural fold Coelom © 2013 Pearson Education, Inc. Somite Intermediate mesoderm 20 days. The neural folds form by folding of the neural plate, which then deepens, producing the neural groove. Three mesodermal Lateral plate aggregates form on each side of the notochord (somite, mesoderm intermediate mesoderm, and lateral plate mesoderm). Figure 28.12c Neurulation and early mesodermal differentiation. Surface ectoderm Neural crest Neural tube Somite Notochord © 2013 Pearson Education, Inc. 22 days. The neural folds have closed, forming the neural tube which has detached from the surface ectoderm and lies between the surface ectoderm and the notochord. Embryonic body is beginning to undercut. Figure 28.12d Neurulation and early mesodermal differentiation. Neural tube (ectoderm) Somite Dermatome Myotome Sclerotome Kidney and gonads (intermediate mesoderm) Epidermis (ectoderm) Gut lining (endoderm) Lateral plate mesoderm • Limb bud • Smooth muscle of gut • Visceral serosa Peritoneal cavity (coelom) © 2013 Pearson Education, Inc. • Parietal serosa • Dermis End of week 4. Embryo undercutting is complete. Somites have subdivided into sclerotome, myotome, and dermatome, which form the vertebrae, skeletal muscles, and dermis respectively. Body coelom present. Figure 28.13 Flowchart showing major derivatives of the embryonic germ layers. Epiblast ECTODERM MESODERM Notochord Somite Intermediate mesoderm ENDODERM Lateral plate mesoderm Somatic mesoderm • Epidermis, hair, nails, glands of skin • Brain and spinal cord Nucleus pulposus of intervertebral discs • Neural crest and derivatives (e.g., cranial, spinal, and sympathetic ganglia and associated nerves; chromaffin cells of the adrenal medulla; pigment cells of the skin) © 2013 Pearson Education, Inc. • Sclerotome: vertebrae and ribs • Dermatome: dermis of dorsal body region • Myotome: trunk and limb musculature • Kidneys • Parietal serosa • Gonads • Dermis of ventral body region • Connective tissues of limbs (bones, joints, and ligaments) Splanchnic mesoderm • Wall of digestive and respiratory tracts (except epithelial lining) • Visceral serosa • Heart • Blood vessels Epithelial lining and glands of digestive and respiratory tracts Effects of Pregnancy: Anatomical Changes • Uterus expands, occupying most of abdominal cavity • Ribs flare to widen thorax • Relaxin causes pelvic ligaments and pubic symphysis to relax to ease birth passage – secreted by the placenta Effects of Pregnancy: Anatomical Changes • Good nutrition vital: 300 additional daily calories • Multivitamins – folic acid reduce fetal risk of neurological problems (spina bifida, anencephaly, and spontaneous preterm birth) • Poor fetal environment may not show for decades later – Below-normal birth rate increases risk of type2-diabetes (women) and cardiovascular disease (men and women) Effects of Pregnancy: Metabolic Changes • Placental hormones – Human placental lactogen (hPL) – maturation of breasts, fetal growth, and glucose sparing in mother (reserving glucose for fetus) – thought to be the cause of gestational diabetes in 10% pregnant women Effects of Pregnancy: Metabolic Changes • Parathyroid hormone and vitamin D levels high throughout pregnancy – Mutivitamin generally includes calcium – adequate calcium for fetal bone mineralization • Remember: bone is site for Ca2+ storage and will be removed regardless of bone integrity Effects of Pregnancy: Physiological Changes • GI tract – Morning sickness believed due to elevated levels of hCG, estrogen and progesterone • Urinary system – Urine production due to maternal metabolism and fetal wastes Effects of Pregnancy: Physiological Changes • Respiratory system – Estrogens may cause nasal edema, congestion and nose bleeds – Tidal volume increases • respond for greater need for oxygen • progesterone enhances sensitivity of the medullary respiratory center to CO2 Effects of Pregnancy: Physiological Changes • Cardiovascular system – Blood volume increases 25–40% – Safeguards against blood loss during childbirth – Cardiac output rises as much as 35-40% • Propels greater volume around body – Venous return from lower limbs may be impaired, resulting in varicose veins Parturition • Giving birth to baby • Labor – Events that expel infant from uterus – Series of steps for induction Events for Labor • Fetal cortisol simulate placenta to release large amounts of estrogen • Increased production of surfactant protein A (SP-A) by fetal lungs trigger inflammatory response in the cervix – occurs weeks before delivery – stimulates its softening in preparation Rise of Estrogen • Three important consequences: – Stimulates myometrial cells to form oxytocin receptors – Promotes formation of gap junctions between uterine smooth muscle – Antagonizes progesterone's influence on uterine muscle • Result: Myometrium becomes irritable and weak – cause of false labor Initiation of Labor • Fetus determines own birth date – Fetal secretion of cortisol stimulates placenta to secrete more estrogen – Rise of estrogen has its effects – Fetal oxytocin causes placenta to produce prostaglandins – Oxytocin and prostaglandins - powerful uterine muscle stimulants – leads to Braxton Hicks contractions in uterus Figure 28.17 Hormonal induction of labor. Start Estrogen Oxytocin from placenta from fetus and mother's posterior pituitary Induces oxytocin receptors on uterus Stimulates uterus to contract Stimulates placenta to release (+) Prostaglandins Stimulate more vigorous contractions of uterus © 2013 Pearson Education, Inc. Positive feedback (+) Delivery Events • Cervix thins and dilates fully to 10 cm • Amnion ruptures, releasing amniotic fluid – “water breaking” • Engagement occurs – head enters true pelvis – head rotates to navigate body through pelvis Delivery • Crowning – when largest dimension of head distends vulva • Episiotomy may be done to reduce tearing – also easier to repair and heal • Once head has been delivered, rest of body delivered much easier Delivery Positions • Vertex position – head-first – Skull dilates cervix; early suctioning allows breathing prior to complete delivery • Breech position – buttock-first – Delivery more difficult; often forceps required, or C-section (delivery through abdominal and uterine wall incision) But wait, there’s more! • Strong contractions continue – detachment of placenta and compression of uterine blood vessels – Delivery of afterbirth (placenta and membranes) occurs ~30 minutes after birth • All placenta fragments must be removed to prevent postpartum bleeding Apgar Score • Neonatal period – four-week period immediately after birth – infant must adjust to dramatic environmental changes • Physical status assessed minutes after birth – 0–2 points each: – Heart rate, Muscle tone, Respiration, Reflexes and Color • Score of 8–10 - healthy Baby’s First Breath • CO2 in body due to loss of placenta – central acidosis which stimulates respiratory control centers to trigger first inspiration • Breathing ain’t easy: – airways tiny; lungs collapsed (never used) • Surfactant in alveolar fluid helps reduce surface tension – occurs in last months – breathing difficulties in premature births Lactation • Production of milk by mammary glands • Toward end of pregnancy – Placental estrogens, progesterone, and human placental lactogen stimulate hypothalamus to release prolactin-releasing factors (PRFs) – Anterior pituitary releases prolactin – mammary glands secrete colostrum Colostrum • Released first 2–3 days – Less lactose but more protein, vitamin A, and minerals; almost no fat • Yellowish secretion rich in IgA antibodies – IgA resistant to digestion; may protect infant against bacterial infection; absorbed into bloodstream for immunity • Followed by true milk production Lactation • Prolactin release wanes after birth • Lactation sustained by mechanical stimulation of nipples - suckling – Suckling causes afferent impulses to hypothalamus – Prolactin stimulates milk production – oxytocin activates let-down reflex • both mammary glands fill with milk regardless of suckling Advantages of Breast Milk • Fats and iron better absorbed; amino acids more easily metabolized as compared with cow's milk or formula – some formula contains high fructose corn syrup and linked to obesity in infants • Beneficial chemicals – IgA, complement, lysozyme, interferon, and lactoperoxidase (protect from infections) – Interleukins and prostaglandins prevent inflammatory responses – Glycoprotein deters ulcer-causing bacterium from attaching to stomach mucosa Lab for Today • Exersise 43 – Understand the steps of spermatogenesis and oogenesis – Understand the menstrual cycle (pg. 652) • Exercise 44 – Understand human development and placental structure