Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
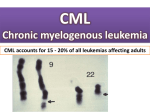
Here are some CML slides that may be helpful for your presentation. Chronic Myeloid Leukemia (CML) Accounts for 15-20% of adult leukemias Median age is 50-60 years Higher incidence noted in patients with heavy radiation exposure In 1960, Nowell and Hungerford detected the Philadelphia chromosome (22q-). In 1973, Rowley identified the reciprocal translocation involving chromosome 9 : t(9;22)(q34;q11). In 1980s, the unique fusion gene termed BCR-ABL was discovered. Epidemiology of CML Median age range at presentation: 45 to 55 years Incidence increases with age Up to 30% of patients are >60 years old Slightly higher incidence in males Male-to-female ratio—1.3:1 At presentation 50% diagnosed by routine laboratory tests 85% diagnosed during chronic phase Sawyers CL. N Engl J Med. 1999;340:1330-1340. Faderl S, et al. Ann Intern Med. 1999;131:207-219. CML: Peripheral Blood Smear Normal Chronic phase CML Courtesy of John K. Choi, MD, PhD, University of Pennsylvania. Pathogenesis of CML A single, pleuripotential, hematopoietic stem cell acquires a Ph chromosome carrying the BCL-ABL fusion gene proliferative advantage Constitutive expression by leukemic stem cell of growth factors ( Il-3, G-CSF) CML cells survive longer due to defective apoptosis Close proximity of the BCR and ABL genes in hematopoietic cells in interphase may favor translocations. Transformation from the chronic phase to blast phase is associated with additional molecular changes ( activation of oncogenes or deletion of tumor-suppressor genes) Pathogenesis of CML The classic BCR-ABL gene result from the fusion of parts of two normal genes ABL on Ch9 and BCR on Ch22. Both genes are ubiquitously expressed in normal tissue,but their precise functions are not well defined. Break occurs in ABL upstream of exon a2 and the major breakpoint cluster region of the BCR gene a 5’ portion of BCR and a 3’ portion of ABL are juxtaposed on a shortened Ch22. The mRNA molecules transcribed from this hybrid gene contain one of two BCR-ABL junctions: e13a2 and e14a2 translated into p210BCR-ABL Pathogenesis of CML What causes the leukemogenic potential of p210bcr-abl? The constitutive activation of the ABL tyrosine kinase activity by BCR deregulated cellular proliferation decreased adherence of leukemic cell to the stroma reduced apoptotic response to mutagenetic stimuli Most crucial domain : the tyrosine kinase encoded by the SRC-homology 1 (SH1) domain on ABL Various substrates have been found to bind to BCRABL and to be tyrosine –phosphorylated by it. The Translocation of t(9;22)(q34;q11) in CML Faderl, S. et al. N Engl J Med 1999;341:164-172 Molecular Targets Target for inhibition: Tyrosine kinase Aim: to design a small chemical compound that would compete with ATP for its binding site in the kinase domain. By blocking the ATP site, no phosphate groups would be transferred to tyrosine residues on the BCR-ABL substrate unphosphorylated substrate protein would not be able to undergo a conformational change to allow it to associate with downstream effectors the downstream reactions would then be impeded interrupting transmission of the oncogenic signal to the nucleus. Molecular Targets Imatinib Mesylate (Gleevec, STI571): a small molecule that inhibits the kinase activity of all proteins that contain ABL, ABL-related gene protein, PDGFR, as well as c-kit receptor. It was first approved in 2001. It occupies the ATP binding site in the SH1 domain of the BCR-ABL oncoprotein. It inhibits cellular growth and induces apoptosis. Other targeted therapies being investigated: The more specific Tyrosine Kinase inhibitors such as the dual SRC-ABL inhibitor : Dasatanib which was approved in June by the FDA. Translocation Leading to the Philadelphia (Ph) Chromosome and the Role of BCR-ABL in th Pathogenesis of CML (Panel A) and the Effect of Normal (Panel B) and Abnormal (Panel C) cFunction on Platelet-Derived Growth Factor and Gastrointestinal Stromal Tumors Savage, D. G. et al. N Engl J Med 2002;346:683-693 Mechanism of Action of BCR-ABL and of Its Inhibition by Imatinib Savage, D. G. et al. N Engl J Med 2002;346:683-693 Clinical Course: Phases of Untreated CML Chronic phase Median duration 5–6 years Advanced phases Accelerated phase Blast crisis Median duration 6–9 months Median survival 3–6 months p53, Rb, p16, t(3;21), t(8;21), t(7;11) Faderl S, et al. Ann Intern Med. 1999;131:207-219. Pasternak G, et al. J Cancer Res Clin Oncol. 1998;124:643-660.