Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
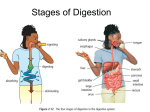
Laura Habighorst RN CAPA Heartland Regional SGNA April 27, 2011 Objectives Identify common GI disorders that require surgical intervention 2. Describe common surgical procedures performed for GI disorders 3. Identify complications associated with surgical interventions 4. Discuss nursing interventions related to treating patients who have undergone surgery for GI disorders. 1. Gastroenterology Nursing: A Core Curriculum, 2008. Chapter 32: Surgical Interventions Esophageal Disorders Most common esophageal GI conditions requiring surgical intervention include: GERD Achalasia Esophageal Cancer Perforation of the Esophagus GERD Indications for Surgery Failure of medical management to treat GERD symptoms, resulting in Barretts, bleeding, aspiration pneumonia, or exacerbation of pulmonary disorders Infants with severe reflux resulting in failure to thrive GERD Surgical Interventions Nissen fundoplication: Performed laparoscopically or open. The gastric fundus is wrapped 360 degrees around the distal esophagus and sutured into place; increasing the tone of the lower esophageal sphincter. Complications: inability to burp or vomit; “Gas Bloat Syndrome” which includes distention, inability to vomit, abdominal pain, severe irritability; slipped or failed surgery occurring in 0.9 – 13% of patients GERD Other surgical procedures Jejunal feeding tube placement Belsey Mark IV repair Hill Posterior Gastropexy Ongoing research therapies Injectable LES implants Gastric placations (enhances the LES) Radiofrequency energy application to the LES Endoscopic valvuloplasty (intussusception of the GE junction into the stomach) Achalsia Achalasia is the absence of peristalsis of the esophageal body and increased LES pressures Indications for Surgery Inadequate response to theraputic (slow eating, chewing well, increased fluids during meals, and sitting up to eat), medical management (esophageal dilatation and botox injections) Achalasia Surgical Intervention Heller’s Myotomy: Performed laparoscopically or open. Laparoscopic approach favored R/T shorter hospital stay, decreased risk of post op GERD, improved esophageal emptying, and fewer episodes of dysphagia. Surgical procedure is described as follows: “Surgical incisions are made to the anterior and posterior portions of the distal esophageal musculature extending into the gastric cardia. The muscle tissue is then divided longitudinally to the mucosal layer allowing for relaxation of the lower esophagus.” May also see a Nissen performed at the same time to decrease possibility of reflux. Esophageal Cancer Surgical intervention requires accurate and careful staging performed typically by endoscopic ultrasound. Surgical resection is treatment of choice for tumors involving the distal two-thirds of the esophagus. Surgical resection has demonstrated cure rates of 5-20% at 3-5 years post diagnosis. Questions remain regarding the use of chemotherapy and radiation to prolong and improve cure rates. Esophageal Cancer Surgical Intervention Surgical removal of esophageal cancer is accomplished by “an abdominal incision…and the stomach and duodenum are mobilized. The thoracic esophagus is then identified and the diseased area excised. An esophageal replacement procedure maybe indicated… There is usually a gastric pull-through that attaches the stomach to the proximal esophagus.” Esophageal Cancer Complications include recurrence of cancer at the anastomotic sites, esophageal stricture, GERD, and dysphagia. Treatment for complications include esophageal dilatation Other Treatment Options Endoscopic Mucosal Resection (EMR): use of saline submucosally to raise the affected area and then resection of it through the use of a specialized cautery loop technique. Perforation of the Esophagus Causes: use of esophageal instrumentation, surgery, foreign body, penetrating trauma, ulcers, ingestion of caustic substances, infections (Herpes Simplex Virus or TB), malignancy, vascular abnormalities (aortic aneurysm, aberrant right subclavian artery) and Boerhaave’s Syndrome ( thoracic esophagus is torn completely away from the gastric cardia) Perforation of the Esophagus Symptoms Cervical perforation: neck pain, muscle spasm, cervical motion pain, dysphonia, hoarseness, and cervical dysphagia Thoracic perforation: dysphagia, odynophagia, dyspnea, cyanosis, chest discomfort Other symptoms may include fever, abdominal rigidity, increased heart rate and increased respiratory rate. Hypotension is a “late and ominous sign if impending shock and circulatory collapse.” Perforation of the Esophagus Treatment Stabilization of respiratory status Antibiotics Volume replacement, TPN Chest tube placement and drainage Surgical repair with suture then pleural, intercostal, or diaphragmatic flaps (used in distal injuries of the esophagus) Perforation of the Esophagus Complications Dependent upon size of tear and repaired area Dysphagia Airway difficulties GERD Esophageal stricture Other Conditions of the Esophagus Esophageal atresia (EA): esophagus ends in a blind pouch; congenital malformation; slightly more common in boys; occurs 1 in 4000 births; associated with tracheoesophageal fistula (open communicating channel between the trachea and esophagus) in 85% of cases. Treated by surgical ligation of the TEF and end to end anastomosis of the esophagus via right thoracotomy, or self-expanding removable stents or adhesives. Complications include dysphagia, anastomotic leak, recurrent TEF, GERD, esophageal stricture, respiratory compromise, inability to manage respiratory secretions. Stomach Disorders Most common disorders of the stomach requiring surgical intervention include: Hiatal hernia Morbid obesity Peptic ulcer disease Perforated peptic ulcer Pyloric stenosis Gastric cancer Hiatal Hernia Sliding Hiatal Hernia Most common approximately 95% Widening of the hiatal tunnel and laxity of the phrenoesophageal membrane, allowing a portion of the gastric cardia to “slide” or herniate upwards Paraesophageal Hernia 5% of hernias GE junction remains in place but the gastric fundus is the leading part of the herniation. Very large and other organs (small intestine, spleen, or colon) may herniate as well. Hiatal Hernia Surgical repair includes “reduction of the herniated portion of the stomach through an abdominal incision and hiatal repair with sutures” and/or mesh. The GE junction is fixed beneath the diaphragm. Fundoplication is generally included. Morbid Obesity Two types procedures currently being performed Vertical banded or silastic ring gastroplasties (Lap-Band™) Roux- en-Y Gastric Bypass Morbid Obesity Vertical banded gastroplasty: a staple line is placed across the fundus and to the lesser curvature of the stomach; thereby reducing stomach capacity and creating a sensation of fullness. Less popular now r/t outlet obstruction and fistulization of the suture line. Silastic ring (Lap-Band™): a laparoscopic procedure in which a silastic ring is placed at the top of the stomach creating a pouch. The opening is adjustable via a subcutaneous port and saline injection under fluoroscopy or in the physician’s office. Morbid Obesity Roux-en-Y Gastric Bypass: performed primarily laparoscopically. The small intestine is divided 15-40 cm downstream from the Ligament of Treitz and Roux limb will attach to the gastric pouch. A pouch (approx 15-20 ml in size) is created at the base of the esophagus in the stomach and the jejunum is then brought up to the stomach pouch. The distal limb anastomoses to the pouch and the proximal limb to the small bowel. Morbid Obesity Complications of weight loss surgery include malabsorption syndromes including iron deficiency anemia, lactose intolerance, “dumping syndrome”, excessive weight loss, diarrhea, perforation, anastomotic ulcers and stenosis, ulceration of the band into the lumen of the stomach. Patient education should include careful dietary instruction and vitamin supplements. Peptic Ulcer Disease Typically able to be treated conservatively with the discovery of H. Pylori and the role of aspirin and NSAIDS in the development of antral and duodenal ulcers. Surgery indicated in emergency situations and when not responsive to conservative treatments Peptic Ulcer Disease Three types of surgery: Partial gastrectomy to reduce number of parietal cells in the stomach decreasing acid production Antrectomy to abolish the gastric phase of secretion and to promote gastric emptying Selective vagotomy to negate the cephalic phase of secretion and to reduce parietal cell sensitivity to secretory stimulus Peptic Ulcer Disease The three specific surgeries are: Billroth I: the distal portion of the stomach, pylorus, and duodenal bulb is removed and the duodenum is reattached by anastomosis with the remaining portion of the stomach Billroth II: the distal portion of the stomach and a portion of the proximal duodenum is resected. The remaining proximal duodenum is closed and a segment of the proximal jejunum is attached to the gastric remnant with an end-to-end or side-to-side anastomosis. Peptic Ulcer Disease Vagotomy: frequently included with both Billroth procedures. When a truncal vagotomy is performed, a complete denervation of the stomach as well as the gallbladder occurs. A “highly selective vagotomy” may be performed which interrupts the nerve fibers to the antrum but preserves the innervation of the pylorus resulting in decreased acid production but motility is maintained. Peptic Ulcer Disease Complications of the surgeries include: Weight loss Iron deficiency anemia Macrocytic anemia Reflux gastritis Diarrhea Perforation of Peptic Ulcer Signs and symptoms: Generalized epigastric pain, with pain referral to the shoulder Abdominal tenderness with guarding, rigidity Absent bowel sounds and progressive abdominal distention Diagnosis made by acute abdominal x-ray series and findings of free air under the diaphragm and air-fluid levels in loops of the small bowel. Perforation of Peptic Ulcer Surgical treatment maybe laparoscopic or open in nature with repair of the perforation by suture, omental pouch or fibrin fixatives. The potential exists for any of the previous discussed surgeries to occur dependent upon the extent of the perforation Pyloric Stenosis Common disorder in infants: Occurrence 3 in 1000 live births in US; 4:1 male and Caucasion dominant Symptoms include projectile, nonbilious emesis leading to dehydration, metabolic alkalosis, and malnutrition Diagnosed with upper GI series or ultrasound Surgical intervention includes pyloromyotomy (incision of the muscle surrounding the pylorus via open abdominal incision) Pyloric Stenosis In adults occurs as a result of chronic ulceration and scarring of the pyloric channel and duodenum Non-surgical treatment includes dilatation Surgical treatment includes truncal vagotomy and Billroth I Gastric Cancer Surgical resection only treatment offering long term chances of survival Extent of surgery dictated by location and size of tumor EUS helpful in determining the type of surgery required EMR is indicated when cancer is confined to mucosal layer of the stomach and without lymph node involvement Wedge resection maybe performed as well Gastric Cancer Total gastrectomy indicated for the following: Length of neoplasm is less than required to obtain clear margins Lesion involves 2 0r 3 sections of the stomach Wide spread cancer May also include a Roux-en-Y procedure Billroth I indicated for the following: Cancers in the distal portion of the stomach Pancreatic Disorders Chronic pancreatitis Resection is performed because it is believed to decrease or eliminate pain Indications include severe pain impacting quality of life and persistent pain despite abstinence of alcohol and administration of nonopioid analgesics. Surgical options include distal pancreatectomy, Whipple procedure with subtotal pancreatectomy, or total pancreatectomy (least performed), pancreaticduodenectomy (causes fewer metabolic deficiencies) Resection maintains drainage of ducts of Wirsung and Santorini as well as tributary ducts within the head of the pancreas Pancreatic Disorders Pancreatic cancer Only 50% of pancreatic cancer patients are free of metastases and only 20% have a curable resectable cancer Most common procedure is Whipple’s procedure or pancreaticoduodenectomy : removal of 50% of the stomach, all of the duodenum and proximal jejunum, resection of the pancreatic head, neck, and uncinate process and the gallbladder and biliary tree. Modified Whipple’s leaves stomach and 2-4 cm of the proximal duodenum (preserves acid inhibiting hormones thus preventing post-op ulcers) Pancreatic Disorders Pancreatic cancer (continued) Third option for surgery is pylorus preserving pancreaticoduodenectomy: the second, third and fourth portions of the duodenum; the neck, head, and uncinate process of the pancreas; and gallbladder and distal biliary tree are removed. Three anastomoses are required : end-to-end pancreaticojejunostomy, an end-to-end hepaticojejunostomy, and end-to-end duodenojenuostomy The Hope for Cancers of the Stomach and Pancreas Endoscopic Ultrasound holds the best hope for early detection and treatment for gastric and pancreatic cancers. “Early diagnosis and accurate staging allows planning for optimal care and greater chance for survival.” Biliary Tract Disorders Cholecystitis as a result of cholelithiasis is the most common indicator for surgery of the biliary tract – cholecystectomy more often done laparoscopically than open. ERCP may be indicated before or after cholecystectomy when stones are identified in the duct by cholangiogram Procedures than maybe performed during open cholecystectomy include choledochostomy(opening of the CBD to explore for stones for obstruction), sphinceroplasty (intractable obstruction or stricutre of the ampulla), and choledochoenterostomy (a side-to-side anastomosis of the CBD to the first part of the dupdenum when the gallbladder has already been removed and obstruction of the CBD continues to occur) Small Intestine Disorders Resection of Small Intestine occurs for multitude of reasons: Congenital anomalies, ie. duodenal atresia, jejunal atresia, ileal atresia, gastrochisis, omphalocele For infants, necrotizing enterocolitis For children and adults, trauma, obstruction, infection, ischemia, or Crohn’s Disease Resection is the removal of the affected area and end-to-end anastomosis; but when the length of the affected area or poor tissue integrity is present, a temporary or permanent ostomy may be required. Small Intestine Disorders Complications that may occur as result of small bowel resection include: Stricture Adhesions and scarring Diarrhea Malnutrition Degree of malnutrition depends upon length of resection and location May require total parenteral nutrition Small Intestine Disorders Surgery for Crohn’s Disease is not entered into lightly and only occurs in those patients not responding to aggressive medical treatment. Indications include: intestinal obstruction, fistula, abscess, uncontrolled hemorrhage, perforation, and failure to thrive in children. Ileostomy may be performed in the presence of severe sepsis related to anorectal Crohns, with or without abscess. Complications associated with Crohns resection include: diarrhea, weight loss, and recurrence of disease. Colon and Rectal Disorders Indications for surgical intervention in the colon and rectum include: Congential anomalies Trauma Inflammatory disease Neoplastic disease Common disorders requiring surgery include: Hirschsprung’s Crohns Ulcerative colitis Colorectal cancer Perforation Hirschsprung’s Disease Incidence 1 in 5000 live births with male dominance Congential absence of intramural ganglia (resulting in loss of motor function) in the intestinal tract most frequently of the anorectum and various lengths within the distal colon Treatment involves removal of the affected area Hirschsprung’s Disease Three surgical types Rectosigmoidectomy (Swenson’s procedure): removal of the rectum and anastomosis of the normal bowel to a 1-2 cm rectal cuff Retrorectal transanal pull-through (Duhamel’s procedure): the aganglionic rectum is left in place and the normal bowel is pulled down behind the rectum and through an incision in the posterior rectal wall at the level of the internal sphincter Endorectal pull-through (Soave’s procedure) Hirschsprung’s Disease Complications of the surgery include: Anal stenosis Obstructive symptoms Fecal incontinence Constipation Enterocolitis Inflammatory Bowel Disease Crohns and ulcerative colitis both affect the large bowel, but only ulcerative colitis affects the large bowel. For ulcerative colitis, surgery is the only definitive cure for the disease. Inflammatory Bowel Disease Indications for colectomy include: Uncontrolled hemorrhage Severe colitis refractory to aggressive medical therapy Toxic megacolon Stricture Perforation Persistent symptoms despite high dose corticosteroid therapy Progression of disease or new onset of complications while on maximum medical therapy Significant treatment related complications Possible malignant stricture or fistula in patients with Crohns Inflammatory Bowel Disease Elective colectomy may occur under the following conditions: Prolonged dependence on steroids Complications related to steroid use Growth retardation despite nutritional support Sexual maturation Epithelial dysplasia (increased risk for carcinoma) Inflammatory Bowel Disease The surgical procedures required for UC include the following procedures: Abdominal colectomy Rectal mucosectomy Endorectal ileoanal pull-through (c/i for Crohns) Anastomosis The above are performed in the following stages: Colectomy Ileoanal anastomosis with creation of rectal pouch Diverting ileostomy Closure of ileostomy after 2-6 months and confirmation of rectal tone as evidenced by manometry Inflammatory Bowel Disease Complications associated with these surgeries include Diarrhea Perianal irritation Incontinence Anastomotic strictures Inflammation of the rectal pouch (pouchitis) Colorectal Cancer Surgical intervention requires removal of the adjacent mesentary, 12 regional lymph nodes, and affected segment of the colon Right hemicolectomy indicated for cancers in the cecum and ascending colon Left hemicolectomy indicated for cancers in the splenic flexure Anterior resection indicated for cancers in the sigmoid or rectosigmoid area Perforation of the Colon May occur as a result of acute inflammatory bowel disease, inserted foreign bodies, penetrating trauma including both endoscopic and surgical in nature. Potentially life-threatening requiring prompt recognition and intervention including surgery. Those most at risk for perforation in the endoscopy lab are those who take immunosuppressive medications Perforation confirmed by x-ray demonstrating free-air under the diaphragm Perforation of the Colon Signs and symptoms include: Fever Abdominal or rectal pain Abdominal distention and rigidity Increased heart rate Increased respiratory rate Hypotension is late sign and indicative of impending shock and circulatory collapse Perforation of the Colon Treatment includes: Stabilization of respiratory status Antibiotic therapy Resuscitative measures, ie. fluid replacement Surgery including closure of the perforation with sutures and irrigation of the abdominal cavity Complications include: Anastomotic strictures Bowel incontinence Anal strictures Transgastric Surgery NOTES procedures Natural Orifice Transluminal Surgery Potential procedures include tubal ligation, oophorectomy, cholecystectomy, gastrojejunostomy, and appendectomy Who will come first - surgeon or the gastroenterologist? THANK YOU!!!!!! WHOOH! NOW WE ARE DONE!!