Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
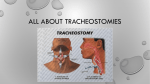
PAEDIATRIC RESPIRATORY REVIEWS (2006) 7, 169–174 MINI-SYMPOSIUM: TRACHEOSTOMY IN CHILDREN Surgical aspects of tracheostomy in children Lesley-Ann Cochrane* and C. Martin Bailey Department of Paediatric Otolaryngology, Great Ormond Street Hospital for Children, Great Ormond Street, London WC1N 3JH, UK KEYWORDS paediatric; tracheostomy; tracheostomy tube; surgery; complications; decannulation; upper airway obstruction Summary Tracheostomy involves the surgical formation of a stoma between the trachea and the skin. It is classically thought of as a treatment to alleviate airway obstruction; however, its clinical applications are varied and include long-term ventilatory support, being an aid in pulmonary toilet and use as a covering procedure during airway surgery. In this article, we review the surgical aspects of tracheostomy, including preoperative considerations, tracheostomy tube choice, operative technique and postoperative complications. Postoperative care of the child with a tracheostomy will also be discussed. ß 2006 Elsevier Ltd. All rights reserved. INTRODUCTION For example, some patients with subglottic stenosis are candidates for a single-stage laryngotracheal reconstruction procedure, which definitively corrects the stenosis without the need for a tracheostomy. Prior to contemplating any surgical procedure, all patients should have their medical management maximised; in particular, gastro-oesophageal reflux disease should be treated aggressively with antireflux medication. Oedema or swelling of the airway may respond to a short course of corticosteroids. The term ‘tracheostomy’ is derived from the Greek stomoun, meaning to create an opening.1 Tracheostomies have been performed from ancient times for a wide variety of clinical conditions. Historically, the most common indication was for the alleviation of upper airway obstruction secondary to infections such as diphtheria or epiglottitis.2–4 With the advent of modern medicine, we have seen a shift in its clinical application, but it continues to be a relatively common procedure in the paediatric tertiary care setting. ANAESTHESIA INDICATIONS Tracheostomies are performed for a variety of reasons. The most common indication for tracheostomy placement is for long-term ventilatory support.2 4 Other indications include alleviation of airway obstruction, as an aid in pulmonary toilet and as a covering procedure during airway or head and neck surgery.1–4 Developments in airway surgery over the last 20 years have provided an alternative to tracheostomy for some causes of upper airway obstruction (Table 1). * Corresponding author. Tel.: +44 207 813 8220; Fax: +44 207 829 8644. E-mail addresses: [email protected] (L.-A. Cochrane), [email protected] (C.M. Bailey). 1526-0542/$ – see front matter ß 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.prrv.2006.06.005 Paediatric tracheostomy is generally performed under general anaesthesia in the controlled environment of the operating theatre. Patients are usually endotracheally intubated for the procedure, but if necessary a rigid ventilating bronchoscope may be used to maintain the airway instead. Alternatively, a laryngeal mask airway or facemask may be used in children when intubation is not possible. In very rare cases, it may be necessary to perform the procedure using local anaesthesia only. Percutaneous dilatational tracheostomy is not suitable for the paediatric population: the landmarks needed to perform the procedure are often difficult to palpate in children as the trachea is soft and flexible, and furthermore the airway is small and often very precarious.5 170 Table 1 L. A. COCHRANE AND C. M. BAILEY Techniques to avoid tracheostomy Type of lesion Technique Subglottic stenosis Single-stage laryngotracheal reconstruction Single-stage open excision Aryepiglottoplasty Cricoid split Subglottic haemangioma Laryngomalacia Failed neonatal extubation should be corrected for size in children with small stature).1 Patients should be fitted with a tube that is appropriate for their age based on the width and length of the trachea. A sizing chart is shown as Table 2.6 Children under the age of 1 year should generally be fitted with a neonatal length tube; older children should be fitted with a paediatric length. For detailed information on tracheostomy tube selection, see another article of this mini-symposium. TRACHEOSTOMY TUBE SELECTION OPERATIVE TECHNIQUE There are many different manufacturers, models and sizes of tracheostomy tube, each with their own advantages and disadvantages.6 Of primary importance when selecting an appropriate tracheostomy tube is the child’s age (which Tracheostomy is performed with the patient lying supine on the operating table. Adequate exposure of the larynx and upper trachea is essential and is best obtained with the neck in a hyperextended position. This can be achieved by placing Table 2 A guide to the size of paediatric tracheostomy tubes, bronchoscopes and endotracheal tubes Reproduced with Permisson from Wyatt et al.6 SURGICAL ASPECTS OF TRACHEOSTOMY IN CHILDREN a sandbag or jelly roll under the patient’s shoulders. If the surgical site is obscured by the soft tissues of the submental area, they can be retracted superiorly with the use of a chinstrap tape, which is secured to the operating room table. The patient’s head is then stabilised by the use of a head ring. The neck is palpated to identify the hyoid bone, thyroid notch and cricoid cartilage. These laryngeal landmarks are marked on the skin as a guide. In neonates, the larynx is high in the neck, and the cricoid cartilage is not easily palpable. The hyoid bone often overrides the upper edge of the thyroid cartilage, making the notch difficult to identify.7 The skin midway between the cricoid and the suprasternal notch is marked and infiltrated with local anaesthetic (1% lignocaine with 1:200 000 adrenaline). A skin incision approximately 2 cm in length is made through the infiltrated area, cutting through fat and platysma. Either a horizontal or a vertical skin incision may be used.8 In infants and small children, a vertical skin incision has traditionally been used. In this age group, the pleural apices may extend superiorly into the neck: a vertical skin incision minimises the need for dissection lateral to the trachea, and thereby reduces the risk of pneumothorax. In older, larger children, this risk is greatly reduced, and a horizontal skin incision is often employed as it is likely to result in a superior cosmetic result. After making the skin incision, a plug of subcutaneous fat is removed with the aid of bipolar diathermy forceps. This step greatly aids in the exposure of deeper tissues and makes it much easier to replace a blocked or displaced tracheostomy tube in the immediate postoperative period.7 The incision is then deepened until the strap muscles are reached. The trachea should be reidentified frequently by palpation in order to avoid inadvertent injury to surrounding structures. The strap muscles are divided in the midline by blunt scissor dissection, allowing them to be separated and retracted laterally, revealing the underlying thyroid isthmus and trachea. The cricoid cartilage lies just superior to the isthmus of the thyroid gland. The cricoid is usually easily visible in older children, but in neonates it is often easier to identify by palpation, feeling for its prominence with fine curved artery forceps. The thyroid isthmus should be separated from the underlying trachea by blunt dissection using fine curved artery forceps and is subsequently divided with bipolar diathermy. In older children with a bulky, vascular isthmus, it may be preferable to divide the isthmus between artery forceps and secure the ends by suture transfixion and ligation. The underlying cricoid cartilage and trachea should then be visible. It is important to identify the cricoid cartilage to prevent inadvertent cannulation at the wrong level. Opening the trachea and tracheostomy tube insertion In children, a vertical incision is generally made in the trachea through the third, fourth and fifth tracheal rings.7 A more superiorly placed incision (i.e. through the second and third 171 tracheal rings) should be avoided in small children if possible, because if the first tracheal ring becomes eroded by pressure from the tracheostomy tube, the cricoid cartilage may then be damaged. Prolene stay sutures are placed on either side of the planned tracheal incision. These are placed to aid in opening the tracheal incision at the time of tracheostomy and are left in place until the first tracheostomy tube change. These sutures facilitate distraction of the tracheal opening in the event that a tube change is required in the early postoperative period before a tract has formed. Once the tracheal incision has been made, the anaesthetist withdraws the endotracheal tube (in the intubated patient) until the tip is just superior to the tracheostome. The tracheostomy tube can then be inserted into the trachea with the aid of its introducer. Once in place, the anaesthetic circuit can be transferred from the endotracheal tube to the tracheostomy tube. In general, it is not necessary to close the skin incision unless it is large. A gap around the tube is essential to allow air escape and prevent postoperative subcutaneous emphysema. A non-adherent dressing is applied to the wound with a keyhole to accommodate the tracheostomy tube. The tracheostomy tube is then secured in place with tapes. These should be tied fairly tightly with the shoulder roll removed and the patient’s neck in a flexed position. At the end of the procedure, the surgeon should auscultate the chest to ensure that there is equal air entry bilaterally: asymmetrical air entry may indicate that the tracheostomy tube is too long and has intubated the right main bronchus, or more rarely that the patient has developed a pneumothorax. ALTERNATIVE SURGICAL TECHNIQUES The placement of maturation sutures between skin and trachea is an optional addition to the standard tracheostomy technique that is becoming more popular. With this technique, size 4.0 absorbable sutures are placed between the superior and inferior aspects of the tracheostomy incision and the skin edges, creating a mature stomal tract.9 Maturation sutures provide an additional safety measure as they allow for easier replacement of a displaced tracheostomy tube in the immediate postoperative period. However, this technique may result in an increased incidence of persistent tracheocutaneous fistula following decannulation. The starplasty procedure is an alternative technique for paediatric tracheostomy described by Koltai, which is based on the geometry of a three-dimensional Z-plasty.10 Cruciform incisions are made in both the skin and the trachea. The resultant triangular flaps are circumferentially interdigitated using size 5.0 absorbable sutures to form a stoma. The tracheostomy site is isolated from the fascial layers that communicate with the pleura, thereby reducing the risk of pneumothorax.10 As with maturation sutures, this technique produces a mature stoma, which makes tube replacement 172 easier. The major disadvantage of this technique is the universal persistence of a tracheocutaneous fistula following decannulation.10 We have described here variations on a standard tracheostomy technique for use in infants and children up to approximately 12 years of age. After the age of 12, the trachea approaches adult size, and conventional adult tracheostomy techniques can be used. COMPLICATIONS Intraoperative complications Bleeding Significant blood loss during tracheostomy is rare. Injury to an abnormally high innominate artery or other anomalous vessel can occasionally occur. This can generally be avoided by careful, controlled dissection of the structures lower in the neck. Pneumomediastinum and pneumothorax The pleural apex rises higher in children than in adults and may extend up into the lower neck. Damage to the cervical pleura may result in pneumothorax or pneumomediastinum. This risk can be minimised by avoiding any dissection lateral to the trachea. Pneumomediastinum and small pneumothoraces are likely to resorb and can be observed, whereas larger pneumothoraces require the insertion of a chest drain.1 Anatomic injury Injury to the oesophagus, cricoid and recurrent laryngeal nerves should not occur in elective tracheostomy.7 Inadvertent damage to the oesophagus can occur if it is mistaken for the trachea. Naso/orogastric tubes should be removed prior to surgery to avoid confusion. L. A. COCHRANE AND C. M. BAILEY antibiotic. Children with long-standing tracheostomies often become colonised with Pseudomonas aeruginosa and/or Staphylococcus aureus.1 Colonisation does not require treatment unless there are signs of acute infection. Subcutaneous emphysema When air leaking around the tracheal incision becomes trapped in the subcutaneous tissues, surgical emphysema ensues. It results from closing the wound too tightly around the tracheostomy tube. If it occurs, the wound should be opened fully. Displacement and blocking of the tracheostomy tube These complications can be avoided by good tracheostomy tube care. New tracheostomies should receive continuous humidification until the first tracheostomy tube change to prevent blockage of the tracheostomy tube. All carers should be trained in how to manage an accidental decannulation or tube blockage, including emergency tracheostomy tube changes as well as cardiopulmonary resuscitation.11 Mortality Tracheostomy-related mortality ranges from 0.5 to 3% in different series.1,12–14 The main causes of death are accidental decannulation and blockage of the tracheostomy tube. POSTOPERATIVE CARE In the immediate postoperative period, a chest radiograph should be performed to ensure that there is no pneumothorax and to check that the tube length is correct, with the tip above the carina.15 The patient must be monitored closely and cared for by appropriately trained nursing staff. Patients should have the following items set up at the bedside:11 Postoperative complications Bleeding Early postoperative bleeding can occur if adequate haemostasis has not been achieved intraoperatively or if there is an unsuspected bleeding diathesis or coagulopathy. Over time, the tracheostomy tube can cause local irritation and inflammation, resulting in a delayed haemorrhage. This risk can be minimised with proper care and adequate humidification. Illfitting metal tracheostomy tubes can cause local erosion of the tracheostome or of the anterior tracheal wall: if left untreated, this can extend to the overlying innominate artery, resulting in a potentially fatal haemorrhage. Infection Local wound infection can occur as in any surgical procedure and is usually easily treated with a short course of oral 1. Emergency kit: a. A spare tracheostomy tube of the same size and brand as that currently in use. b. A tracheostomy tube one size smaller than that currently in use. c. Round-ended scissors. d. Tracheostomy tube tapes. e. Water-based lubricant. f. A length of suction catheter that can be used to railroad in a new tracheostomy tube if required. 2. Suction apparatus and sterile suction catheters with distal and lateral holes at the tip. 3. Humidification. Adequate humidification is essential. During the initial postoperative period, humidified air should be delivered continuously to reduce the tenacity of the secretions and SURGICAL ASPECTS OF TRACHEOSTOMY IN CHILDREN maintain tube patency.11 The tracheostomy tube must be kept clear of secretions by frequent suctioning. Suctioning can be facilitated by the instillation of 0.5 ml sterile normal saline into the tube first. A sterile catheter is then inserted into the tracheal lumen gently, and suction is applied only as the catheter is withdrawn. Tracheostomy tubes are generally changed for the first time after 7 days. The timing of subsequent tube changes is variable, depending upon the type of tracheostomy tube used. Some patients may require more frequent tube changes due to thick secretions, infection or patient preference. Following the first tracheostomy tube change, continuous humidification can be discontinued and a heat and moisture exchanger or ‘Swedish nose’ fitted. DECANNULATION Once the underlying indication for the tracheostomy has resolved or has been corrected, decannulation can be considered. Prior to decannulation, a laryngoscopy and bronchoscopy should be performed to evaluate the airway for granulation tissue, suprastomal collapse or any other problem that might preclude successful decannulation. Once any granuloma or suprastomal collapse has been adequately treated, the patient can be decannulated on the ward.16,17 During ward decannulation, the patient’s tracheostomy tube is gradually down-sized and then blocked off prior to removal. A full decannulation protocol is detailed in Table 3.16,17 Should the child experience respiratory distress at any time, the protocol should be aborted and the tracheostomy re-established. Following a successful decannulation, the stoma is left to heal by secondary intention. Approximately 40% of stomas fail to close completely on their own, leaving a persistent tracheocutaneous fistula.1,12,13,18 If this persists for 6 months or more, it can be closed surgically. Surgical closure of persistent tracheocutaneous fistula Persistent tracheocutaneous fistulas are closed surgically under general anaesthesia. An elliptical skin incision is made around the fistula. Dissection is then carried through the surrounding scar tissue to isolate the tract from the adjacent Table 3 Decannulation protocol Day 1 Down-size to a size 3 tracheostomy tube Day 2 Block the tracheostomy tube for 12 h If successful, continue overnight for a further 12 h If unsuccessful, unblock overnight and repeat the next day Day 3 Decannulate and observe on the ward Day 4 Observe off the ward Day 5 Discharge 173 healthy tissue down to the level of the trachea. After the tract has been completely isolated from surrounding tissues, it is resected from the trachea and the edges are approximated with reabsorbable sutures.18 The strap muscles are also mobilised from the surrounding scar tissue and then reapproximated in the midline over the tracheal closure. The skin and subcutaneous tissues are neatly sutured together. A small Penrose drain can be used to avoid any subcutaneous emphysema, although this is not always necessary. A period of intubation is not required postoperatively. Suprastomal granuloma Suprastomal granuloma formation is common.1,12,13 Granulomas occur in the tracheal lumen at the superior margin of the tracheostome where the mucosa is irritated and inflamed by the tracheostomy tube. Granulomas may also arise at the site of the tracheostomy tube tip, due to either an ill-fitting tube or traumatic suction. Large and obstructing granulomas should be treated prior to decannulation. This can be done via the stoma with punch forceps under bronchoscopic control or endoscopically using a KTP laser.19,20 Suprastomal collapse Some degree of collapse of the anterior tracheal wall just superior to the tracheostome is almost inevitable in longterm paediatric tracheostomies. It results from pressure on the tracheal rings from the tracheostomy tube, with subsequent inflammation, chondritis and eventual weakening of the cartilaginous rings. The degree of collapse is usually mild and does not require any treatment prior to decannulation. More significant collapse requires treatment as it may prevent successful decannulation. Suprastomal collapse causing less than 50% occlusion of the airway can usually be successfully treated endoscopically using a KTP laser to vaporise the collapsing area.20 Collapse causing more than 50% occlusion requires an open surgical decannulation or a formal open stomal reconstruction. Surgical decannulation This is a single-stage procedure in which the tracheostomy tube is removed and the stoma site is surgically closed.21 At the beginning of the procedure, the tracheostomy tube is replaced with an endotracheal tube. The technique involves excising the stoma with an ellipse of skin and carefully dissecting out the fibrous tracheostomy tract down to the opening in the tracheal cartilage. Any intraluminal suprastomal granuloma can be excised in continuity with the tract. The tract is then excised flush with the anterior surface of the trachea, taking care not to remove any tracheal wall. The collapsing portion of the tracheal wall is hitched forward by suturing it anteriorly to the strap muscles on either side.21 This provides constant anterior traction on the collapsed area during healing. Postoperatively, the patient is intubated for a period of 24–48 h. Surgical 174 decannulation is usually reserved for selected cases in which there is moderate suprastomal collapse. Stomal reconstruction Patients with severe suprastomal collapse or stomal stenosis will require a formal stomal reconstruction procedure in order to successfully achieve decannulation. Stomal reconstruction is a single-stage procedure similar to a laryngotracheal reconstruction. The tracheostomy fistula is excised as in a surgical decannulation, leaving a small defect in the trachea at the site of the former tracheostomy. The area of collapse immediately superior to this defect is incised to allow for the placement of a reinforcing graft. A costal cartilage graft is then used to close the tracheostomy defect and to expand and reinforce the area of collapse. The graft is sutured into place with absorbable sutures. A Penrose drain is left in the wound for 48 h to prevent subcutaneous emphysema. Postoperatively, the patient is left intubated for a period of 5–7 days. PRACTICE POINTS Indications for tracheostomy include the alleviation of upper airway obstruction, long-term ventilatory support, as an aid in pulmonary toilet and as a covering procedure for head and neck surgery. Children should have a postoperative chest radiograph to rule out pneumothorax and pneumomediastinum, and to check the position of the tube tip. Prior to decannulation, children with long-standing tracheostomies should undergo a laryngoscopy and bronchoscopy to evaluate for suprastomal granuloma or collapse. A suprastomal granuloma can be removed via the stoma with punch forceps under bronchoscopic control or endoscopically using a KTP laser. Suprastomal collapse causing less than 50% occlusion of the airway can usually be successfully treated with a KTP laser to vaporise the collapsing area. More significant collapse requires surgical decannulation or formal open stomal reconstruction in order to successfully achieve decannulation. Following ward decannulation, up to 40% of children have a persistent tracheocutaneous fistula that requires surgical closure. L. A. COCHRANE AND C. M. BAILEY REFERENCES 1. Goldstein NA. The Care of a Child with a Tracheostomy. Alexandria, VA: American Academy of Otolaryngology-Head and Neck Surgery Foundation Inc., 2004. 2. Hadfield PJ, Lloyd-Faulconbridge RV, Almeyda J, Albert DM, Bailey CM. The changing indications for paediatric tracheostomy. Int J Pediatr Otorhinolaryngol 2003; 67: 7–10. 3. Butnaru CS, Colreavy MP, Ayari S, Froehlich P. Tracheotomy in children: evolution in indications. Int J Pediatr Otorhinolaryngol 2006; 70: 115–119. 4. Kremer B, Botos-Kremer AI, Eckel HE, Schlondorff G. Indications, complications and surgical techniques for pediatric tracheostomies – an update. J Pediatr Surg 2002; 37: 1556–1562. 5. Kost KM. Endoscopic percutaneous dilatational tracheotomy: a prospective evaluation of 500 consecutive cases. Laryngoscope 2005; 115: 1–30. 6. Wyatt ME, Bailey CM, Whiteside JC. Update on tracheostomy tubes. J Laryngol Otol 1999; 113: 35–38. 7. Bailey CM. Tracheostomy. in: Spitz L, Coran AG (eds.), Operative Paediatric Surgery, 6th Edn. (in press). 8. Hotaling A, Robbins W, Madgy D, Belenky W. Pediatric tracheotomy: a review of technique. Am J Otolaryngol 1992; 13: 115–119. 9. Craig MF, Bajaj Y, Hartley BEJ. Maturation sutures for the paediatric tracheostomy – an extra safety measure. J Laryngol Otol 2005; 119: 985–987. 10. Koltai PJ. Starplasty: a new technique of pediatric tracheotomy. Arch Otolaryngol Head Neck Surg 1998; 124: 1105–1111. 11. Cooke J. Tracheostomy: Care and Management. London: Great Ormond Street Hospital Clinical Procedure Guidelines, 2004. 12. Carr MM, Poje CP, Kingston L, Kielma D, Heard C. Complications in pediatric tracheostomies. Laryngoscope 2001; 111: 1925–1928. 13. Midwinter K, Carrie S, Bull P. Paediatric tracheostomy: Sheffield experience 1979–1999. J Laryngol Otol 2002; 116: 532–535. 14. Wetmore RF, Marsh RR, Thompson ME, Tom LW. Pediatric tracheostomy: a changing procedure? Ann Otol Rhinol Laryngol 1999; 108: 695–699. 15. Greenberg JS, Sulek M, de Jong A, Friedman EM. The role of postoperative radiography in pediatric tracheostomy. Int J Pediatr Otorhinolaryngol 2001; 60: 41–47. 16. Waddell A, Appleford R, Dunning C, Papsin BC, Bailey CM. The Great Ormond Street protocol for ward decannulation of children with tracheostomy: increasing safety and decreasing cost. Int J Pediatr Otorhinolaryngol 1997; 39: 111–118. 17. Kubba H, Cooke J, Hartley B. Can we develop a protocol for the decannulation of tracheostomies in children less than 18 months old? Int J Pediatr Otorhinolaryngol 2004; 68: 935–937. 18. Stern Y, Cosenza M, Walner D, Cotton R. Management of persistent tracheocutaneous fistula in the pediatric age group. Ann Otol Rhinol Laryngol 1999; 108: 880–883. 19. Gupta A, Cotton RT, Rutter MJ. Pediatric suprastomal granuloma: management and treatment. Otolaryngol Head Neck Surg 2004; 131: 21–25. 20. Sharp HR, Hartley BE. KTP laser treatment of suprastomal obstruction prior to decannulation in paediatric tracheostomy. Int J Pediatr Otorhinolaryngol 2002; 66: 125–130. 21. Al-Saati A, Morrison GAJ, Clary RA, Bailey CM. Surgical decannulation of children with tracheostomy. J Laryngol Otol 1993; 107: 217–221.