Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
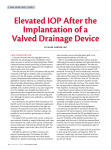
Ahmed Glaucoma Valve and Single-Plate Molteno Implants in Treatment of Refractory Glaucoma: A Comparative Study NADER NASSIRI, GHAZAL KAMALI, MOHAMMAD RAHNAVARDI, BABAK MOHAMMADI, SAMAN NASSIRI, LALEH RAHMANI, AND NARIMAN NASSIRI ● PURPOSE: To report 2-year follow-up data after Ahmed valve implantation (New World Medical, Inc) and Molteno single-plate implantation surgical treatment of refractory glaucoma. ● DESIGN: Prospective, randomized, comparative study. ● METHODS: Patients with refractory glaucoma, defined as uncontrolled intraocular pressure (IOP) of more than 21 mm Hg despite maximal antiglaucoma medication, previously failed nonseton surgical treatment, or a combination thereof were included. Ninety-two patients were allocated randomly to each of the study groups and underwent implantation of either the Ahmed valve implant (model FP7; 184 mm2 surface area) or Molteno single-plate implant (134 mm2 surface area) and were followed up for 24 months. Main outcome measures were IOP and surgical success rate. Other outcome measures were changes in visual acuity, number of ant-glaucoma medications, mean deviation of visual field, and rate of intraoperative and postoperative complications. ● RESULTS: Those who successfully completed the trial (28 in the Molteno group and 29 in the Ahmed group) achieved significantly less IOP and fewer glaucoma medications, but worse visual acuity 24 months after surgery. The Molteno group, compared with the Ahmed group, achieved significantly lower IOPs after the early postoperative period until the end of the study. Both groups reasonably maintained visual field during the follow-up. The rate of surgical failure was comparable in both groups. Median survival time was 24 months for both groups. There were no devastating intraoperative or postoperative complications in either group. ● CONCLUSIONS: Both Ahmed and Molteno implants successfully preserved visual field, although IOP control was more pronounced in the Molteno implant group. (Am J Ophthalmol 2010;149:893–902. © 2010 by Elsevier Inc. All rights reserved.) See Accompanying Editorial on page 875. Accepted for publication Jan 14, 2010. From the Department of Ophthalmology, Imam Hossein Medical Center, Shaheed Beheshti University of Medical Sciences, Tehran, Iran (Nad.N., G.K.); and Vanak Eye Surgery Center, Tehran, Iran (M.R., B.M., S.N., L.R., Nar.N.). Inquiries to Nariman Nassiri, Vanak Eye Surgery Center, No. 41, Haghani Highway, Vanak, Tehran, Iran; e-mail: [email protected] 0002-9394/$36.00 doi:10.1016/j.ajo.2010.01.025 © 2010 BY H ISTORICALLY, GLAUCOMA DRAINAGE IMPLANTS have been reserved for cases of refractory glaucoma deemed at high risk of failure (e.g., eyes with a previous history of failed trabeculectomy1,2 and with neovascular and uveitic glaucoma) with standard filtration surgery. Despite the high-risk profile of these patients, moderately good levels of success with various types of glaucoma drainage implants have been observed. Consequently, the use of these implants has increased in recent years, and they have become the preferred surgical procedure for complex cases.3,4 For more than 2 decades, various types of glaucoma drainage implants have been developed. These implants may be subdivided into valved and nonvalved designs. Those with a nonvalved structure act as an open tube, which may result in immediate postoperative hypotony5,6 and its attendant complications (e.g., flat anterior chamber, suprachoroidal effusion, and suprachoroidal hemorrhage). Hypotony during the immediate postoperative period is less common with valved drainages, although it may still occur.7–10 We investigated the success of the Ahmed valve implant (New World Medical, Inc, Rancho Cucamonga, California, USA) and the Molteno singleplate implant (Molteno Ophthalmic Limited, Dunedin, New Zealand) in treating eyes with refractory glaucoma during a follow-up period of 24 months. METHODS ● STUDY SUBJECTS: A prospective, randomized trial was performed from January 2003 through August 2005 at 3 medical centers, namely, Imam Hossein Medical Center, Negah Eye Hospital, and Vanak Eye Surgery Center, all in Tehran, Iran. The eligibility criteria were refractory glaucoma, defined as uncontrolled intraocular pressure (IOP) despite maximal antiglaucoma medication, previously failed nonseton surgical treatment, or a combination thereof. The exclusion criteria included age younger than 40 years, a visual acuity of no light perception, lens opacity, elevated IOP associated with silicone oil, previous glaucoma drainage device implantation in the same eye, previous cyclodestructive treatment, increased risk of endophthalmitis (e.g., active adnexal and ocular surface infection, immunosuppression, or ELSEVIER INC. ALL RIGHTS RESERVED. 893 Of 101 eligible patients, 92 (91.0%) agreed to participate. Study subjects were assigned randomly to either the Ahmed or Molteno groups. Randomization was performed using a random permuted block design with a block size of 2, stratified for age, sex, and hosting medical center. Neither patients nor investigators were masked to study groups. Figure 1 shows a flow chart of the trial. Operations were all performed by the same senior right-handed surgeon (Nad.N.). To reduce the risk of potentially permanent visual loss, all patients underwent surgery within 4 weeks of enrolling in the trial. Before operation, the exclusion criteria again were reviewed by the surgeon. ● PREOPERATIVE AND POSTOPERATIVE ASSESSMENTS: Presurgical assessments included slit-lamp biomicroscopic examination, funduscopy, Snellen visual acuity (VA), baseline IOP, number of antiglaucoma medications, and Humphrey perimetry results. Follow-up visits were scheduled at day 1, week 1, and months 1, 3, 6, 9, 12, 18, and 24, and more often when necessary. Postoperative evaluations included assessment of visual acuity, IOP (in millimeters of mercury), number of antiglaucoma medications, lens opacity, and postoperative complications. Humphrey perimetry was performed at postoperative months 3 and thereafter. A formal motility evaluation was performed in all patients at baseline and at the 1-year and 2-year follow-up visits, as well as during any visits after 3 months if the patient reported diplopia. The best-corrected visual acuity was measured using a Snellen chart (CP-690; Nidek Co, Ltd, Gamagori Aichi, Japan) calibrated for a 20-foot (approximately 6 m) distance by the line assignment method within the month before the surgery; the figures were converted to logarithm of the minimal angle of resolution notation by the standard conversion table. IOP was measured using a Goldman applanation tonometer (AT-900; Haag-Streit AG, Koniz, Switzerland) mounted on a slit lamp; if required, gonioscopy (Haag-Streit AG) also was performed. The preoperative IOP for each eye was considered as the last measure before operation. 24 –2 threshold visual field assessment was performed with the Humphrey Field Analyzer (Allergan-Humphrey Instruments, San Leandro, California, USA). The mean deviation—a visual field index provided by Statpac-2 (AllerganHumphrey Instruments)13 and determined from a comparison with an age-matched normal population—was available as a global assessment of visual field damage. We considered the phenomenon of learning effect in our analysis of mean deviation; this is a phenomenon whereby the baseline visual field is worse than in subsequent tests,14,15 so using baseline tests may result in a false-positive defect being compared with actual glaucomatous progression or the development of a cataract, and not stable fields. To avoid this, we included only results where consecutive field tests did not show an improvement of 2 dB or more in the mean deviation over the baseline reading. FIGURE 1. Trial flow chart, the Ahmed valve and Molteno implant groups. A ⴝ analyzed; CS ⴝ complete success; F ⴝ intervention failure; L ⴝ lost to follow-up; QS ⴝ qualified success. immunodeficiency, including the use of systemic steroids), posterior segment disorders, or pre-existing ocular comorbidities (e.g., pterygium, phacodonesis, corneal opacity, or corneal endothelial dystrophies). Only 1 eye per patient was included in this trial. An estimation of sample size was performed considering a study power of at least 0.8 with an ␣ error of 0.05 aiming to detect a difference of 1 mm Hg in mean IOP in the postoperative month 24 between the 2 groups. Mean IOP in the postoperative month 24 was estimated to be 15 mm Hg in the Ahmed group based on the results of the previous studies.11,12 Based on this estimation, a total of 64 study subjects was deemed adequate, and considering a total of 30% assumed dropout and failure rate during the follow-up, recruitment of at least 92 study subjects was targeted. 894 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE 2010 ● OUTCOME MEASURES: IOP (primary outcome measure), number of antiglaucoma medications, visual acuity, visual field, and surgical failure were considered as measures assessing efficacy; intraoperative and postoperative complications were considered as measures assessing safety. Surgical failure was defined as persistent IOP of more than 21 mm Hg on maximally tolerated medications or IOP less than 6 mm Hg on 2 consecutive visits, phthisis bulbi, reduction of vision to no light perception, removal of the shunt implant, reoperation for glaucoma, or any devastating intraoperative or postoperative complication.11,16 Reoperation was defined as additional glaucoma surgery requiring a return to the operating room, such as placement of a tube shunt. Interventions performed at the slit lamp, such as needling procedures, were not considered reoperations. Surgical revision of the glaucoma shunt implants for other postoperative reasons (e.g., tube repositioning or repair of conjunctival wound dehiscence) were recorded, but were not considered surgical failures. Devastating complications included suprachoroidal hemorrhage that threatened visual fixation, was likely to develop a kissing appearance, or both; malignant glaucoma; endophthalmitis; retinal detachment; chronic hypotony; or serous choroidal effusions necessitating surgical drainage or that had a kissing appearance. Treatment success was subdivided into complete and qualified. A complete success was defined as IOP between 6 and 21 mm Hg without any antiglaucoma medication, and qualified success was defined as IOP between 6 and 21 mm Hg with 1 medication or more. Hypotony was defined as an IOP of less than 6 mm Hg on 2 consecutive visits;10,12,16 a hypertensive phase was defined as an IOP of more than 21 mm Hg during the first 3 postoperative months (with or without medications) after a reduction in IOP to less than 22 mm Hg during the first postoperative week and not caused by tube obstruction, retraction, or valve malfunction.17 Resolution of this phase was IOP of less than 22 mm Hg along with a reduction of the IOP by 3 mm Hg or more with the same or fewer number of medications, or reduction of at least 1 medication with a change in of IOP less than 3 mm Hg.17 ● PROCEDURE: The tube shunts used were either the valved 184-mm2 surface area Ahmed Glaucoma Valve (AGV Model FP7) or the 134-mm2 surface area single-plate Molteno implant. Before the trial, the surgeon made a transition from the polypropylene (model S2) to the silicone (model FP7) Ahmed valve. Recent studies have reported significantly lower failure rates with silicone valves.18 –21 General anesthesia was given in most cases; in some cases, a peribulbar block consisting of lidocaine 2% (Xylocaine; AstraZeneca, Cheshire, United Kingdom) with hyaluronidase (Hyalase; Wockhardt Ltd, Wrexham, United Kingdom) was used. Immediately before surgery in the operating room, povidone–iodine 5% was applied to the skin of the eyelids of the operative eye, nose, and forehead. The operaVOL. 149, NO. 6 AHMED VALVE VS TABLE 1. Demographic and Baseline Characteristics of Study Subjects from the Ahmed Valve Implant and Molteno Single-Plate Implant Groups Characteristics Ahmed Valve Implant (n ⫽ 46) Molteno Single-Plate Implant (n ⫽ 46) Demographic characteristics Mean age (SEM), yrs 59.4 (1.51) 63.3 (1.62) Male/female, n 25/21 22/24 Background conditions, n (%) Diabetes mellitus 11 (23.9) 11 (23.9) Hypertension 13 (28.3) 13 (28.3) Family history of glaucoma 11 (23.9) 10 (21.7) Bilateral glaucoma 12 (26.1) 14 (30.4) Previous glaucoma treatments, n (%) Penetrating iridectomy 8 (17.4) 9 (19.6) Trabeculectomy 17 (37.0) 18 (39.1) No. of trabeculectomy procedures 1 1 (2.2) 1 (2.2) 2 14 (30.4) 14 (30.4) 3 2 (4.3) 3 (6.5) Enrolled eye baseline features Side, right/left, n 24/22 20/26 Lens group, n (%) Phakic 31 (67.4) 33 (71.7) Aphakic 6 (13.0) 7 (15.2) Pseudophakic 9 (19.6) 6 (13.0) Subtypes of glaucoma, n (%) Failed filtration 17 (37.0) 19 (41.3) Pseudoaphakia 9 (19.6) 6 (13.0) Neovascular 9 (19.6) 12 (26.1) Aphakia 6 (13.0) 6 (13.0) Uveitic 5 (10.9) 3 (6.5) Mean IOP (SEM), mm Hg 32.11 (1.32) 32.41 (1.27) Mean BCVA (SEM), logMAR units 0.64 (0.09) 0.61 (0.09) Visual field mean deviation (SEM), dB –18.57 (0.82) –19.11 (0.79) Mean no. of glaucoma medications (SEM) 2.7 (0.08) 2.7 (0.09) P Value .08 .67 1.00 1.00 1.00 .82 1.00 1.00 .98 .53 .69 .82 .87 .86 .64 .72 BCVA ⫽ best-corrected visual acuity; dB ⫽ decibels; IOP ⫽ intraocular pressure; logMAR ⫽ logarithm of the minimal angle of resolution; SEM ⫽ standard error of mean. tive eye was draped in the usual manner for ophthalmic surgery. In both types of shunts, a clear corneal traction suture was placed with silk 7-0, and the fornix-based conjunctival flap and Tenon capsule were fashioned supratemporally. To prime the valve, the tube of the shunt was irrigated with a balanced saline solution (BSS; Alcon, Fort Worth, Texas, MOLTENO IMPLANT 895 TABLE 2. Preoperative and Postoperative Month 24 Figures in Those Study Subjects from the Ahmed Valve Implant and Molteno Single-Plate Implant Groups Who Successfully Completed the Trial Ahmed Valve Implant (n ⫽ 29) Mean IOP (SEM), mm Hgb Mean BCVA (SEM), logMAR units Visual field mean deviation (SEM), dBc Mean no. of glaucoma medications (SEM) Molteno Single-Plate Implant (n ⫽ 28) Preoperative Month 24 P Valuea Preoperative Month 24 P Valuea 30.81 (1.67) 0.66 (0.12) ⫺19.70 (0.96) 2.8 (0.11) 17.00 (0.23) 0.78 (0.12) ⫺19.67 (0.95) 1.03 (0.27) ⬍0.001 0.001 0.09 ⬍0.001 33.06 (1.66) 0.59 (0.12) ⫺18.45 (1.11) 2.7 (0.11) 15.36 (0.33) 0.70 (0.11) ⫺19.49 (1.17) 1.41 (0.19) ⬍.001 ⬍.001 ⬍.001 ⬍.001 BCVA ⫽ best-corrected visual acuity; dB ⫽ decibels; IOP ⫽ intraocular pressure; logMAR ⫽ logarithm of the minimal angle of resolution; SEM ⫽ standard error of the mean. a Wilcoxon signed-rank test comparisons of postoperative month 24 and preoperative figures in each study group, post hoc study powers for all significant comparisons were ⬎80% (based on an ␣ error of 0.05). b P ⬍ .001, Mann–Whitney U test comparison of postoperative month 24 figures between the 2 study groups. c Three subjects in the Ahmed group and 5 in the Molteno group were excluded from visual field calculations because of the learning effect, reducing total number to 26 in the Ahmed group and 23 in the Molteno group. USA). The plate was secured 8 to 9 mm posterior to the surgical limbus with interrupted 7-0 nylon sutures using tapered cutting needles. In the Molteno implant group, the anterior chamber drainage tube was occluded by tying a 7-0 Vicryl suture (Ethicon, Norderstedt, Germany) around its exterior, where it joined the plate of the implant, to restrict the flow through the device temporarily until encapsulation of the plate occurred. Fenestrations were placed anterior to the suture using a 28-gauge needle to allow leakage of the aqueous, providing initial IOP control. Next, in both groups, the tube was trimmed to extend approximately 2 to 3 mm beyond the surgical limbus with the bevel facing up; it then was entered into the anterior chamber by a 23-gauge needle parallel to the iris plane. If a peripheral iridectomy was present from a previous surgery, the needle tract was placed slightly to one side of the iridectomy. Sodium hyaluronate (Healon, 10 mg/mL; Advanced Medical Optics, Santa Ana, California, USA) was injected to prevent sudden collapse of the anterior chamber. The tube was inserted with smooth forceps through the needle tract, ensuring that no iris or corneal touch occurred. In patients with aphakic and pseudophakic glaucoma who had vitreous in the anterior chamber, an anterior vitrectomy was performed before the placement of the tube. The tube then was anchored to the sclera using a 10-0 nylon suture and was covered with a rectangular piece of donor scleral patch graft. The conjunctiva was closed using 10-0 interrupted nylon sutures. A clear cornea paracentesis then was created to remove the Healon as much as was possible, and the anterior chamber then was reformed with BSS. At the end of surgery, subconjunctival injections of antibiotics and corticosteroids were administered away from the surgical site. No adjunctive antimetabolite was used in any of the cases. Postoperative management consisted of combination topical antibiotic and steroid eye drops, which were tapered over the course of 6 to 8 weeks. Antiglaucoma medications 896 AMERICAN JOURNAL FIGURE 2. Graph showing the mean preoperative and postoperative intraocular pressures in the Ahmed valve and Molteno implant groups. *P < 0.001, **P ⴝ 0.001, ***P < 0.01, Mann–Whitney U test comparisons of the figures at the different time points between 2 groups. were removed or added as needed, depending on the IOP and clinical status of the operated eye. ● STATISTICAL ANALYSIS: Preoperative and postoperative measures were compared within and between study groups. Quantitative variables were compared using nonparametric tests, that is, the Mann–Whitney U test or Wilcoxon signed-rank test, whichever appropriate. The OF OPHTHALMOLOGY JUNE 2010 FIGURE 3. Graph showing the preoperative and postoperative mean number of glaucoma medications in the Ahmed valve and Molteno implant groups. Note that comparisons at all time points between 2 groups were insignificant. FIGURE 4. Graph showing visual acuity in the Ahmed valve and Molteno implant groups. Note that comparisons at all time points between 2 groups were insignificant. logMAR ⴝ logarithm of the minimal angle of resolution. chi-square and Fisher exact tests were used for qualitative variables. To determine factors independently associated with IOP in postoperative month 24, multivariate analysis was performed using a stepwise linear regression model of several variables. The cumulative probability of success was analyzed by Kaplan-Meier life-table analysis. As soon as an VOL. 149, NO. 6 AHMED VALVE VS eye reached a failure end point, it was censored from further analysis. Cox proportional hazards analysis was used to identify independent predictors of surgical failures. Post hoc study power for significant comparisons was calculated using G*Power 3, a power analysis software.22 P values less than .05 were considered statistically significant. MOLTENO IMPLANT 897 TABLE 3. Postoperative Complications after Ahmed Valve Implantation and Molteno Single-Plate Implantation Complications Hyphema ⬎ 1 mm Wound dehiscence Choroidal effusion Choroidal maculopathy Flat anterior chamber Obstruction of tube By fibrin By clot Tenon cyst Cataract formation Ahmed Valve Implant (n ⫽ 46) Molteno Single-Plate Implant (n ⫽ 46) P Valuea 3 (6.5) 2 (4.3) 2 (4.3) 0 (0) 1 (2.2) 2 (4.3) 2 (4.3) 4 (8.7) 1 (2.2) 2 (4.3) 1.00 1.00 .67 1.00 1.00 2 (4.3) 0 (0) 13 (28.3) 5 (10.9) 1 (2.2) 1 (2.2) 11 (23.9) 8 (17.4) 1.00 1.00 .83 .55 Data are presented as n (%). a Fisher exact test. FIGURE 5. Kaplan-Meier survival curve analysis of event-free rates among the Ahmed valve and Molteno implant groups. ● SURGICAL FAILURE AND SURVIVAL ANALYSIS: Both groups were comparable in terms of surgical failures. There were a total of 7 failures (1 failed filtration, 3 uveitic, 1 aphakia, 1 neovascular, and 1 pseudoaphakia) in the Ahmed group at a mean postoperative time of 11.6 ⫾ 4.7 months and 5 failures (1 failed filtration, 1 uveitic, 1 pseudophakia, 2 neovascular) in the Molteno group at a mean postoperative time of 12.0 ⫾ 8.7 months. All surgical failures were the result of uncontrolled glaucoma (IOP ⬎ 21 mm Hg) with the maximally tolerated antiglaucoma medications. Qualified and complete rates of success at 12 months and 24 months after operation were comparable between both groups (Figure 1). In Kaplan-Meier survival analysis, median survival time was 24 months for both the Ahmed and Molteno groups (P ⫽ .65, log-rank test). The cumulative probability of success at 1 and 2 years was 88% and 82% in the Ahmed group, respectively, and 93% and 84% in the Molteno group, respectively (Figure 5). Univariate Cox proportional hazards analysis could not identify any independent predictor of operation failure among several variables tested, including study group (Ahmed vs Molteno) and other variables as listed in Table 1. In multivariate analysis of the same variables, the Ahmed valve (regression coefficient, 1.69; 95% confidence interval, 0.91 to 2.47) and hypertension (regression coefficient, 0.90; 95% confidence interval, 0.02 to 1.79) were associated independently with higher IOP in postoperative month 24. RESULTS BASELINE VARIABLES WERE COMPARABLE IN BOTH GROUPS (Table 1). Those who successfully completed the trial in both groups (28/46 [60.9%] in the Molteno group and 29/46 [63.0%] in the Ahmed group; Figure 1) achieved significantly lower IOP and fewer glaucoma medications, but worse visual acuity 24 months after operation in comparison with their preoperative measures (Table 2). ● INTRAOCULAR PRESSURE AND OTHER EYE FEATURES: IOP was significantly lower in the Ahmed group than in the Molteno group in postoperative day 1 and week 1. Nevertheless, the Molteno group showed markedly lower IOPs thereafter up to the end of the study in postoperative month 24 (Figure 2). The Molteno group, compared with Ahmed group, showed significantly higher mean (⫾ standard deviation) percentages of change from preoperative IOP to postoperative month 12 IOP (⫺50.7 ⫾ 11.6% vs ⫺41.4 ⫾ 13.9%; P ⫽ .004; post hoc study power, 91%) and month 24 IOP (⫺49.7 ⫾ 11.6% vs ⫺41.9 ⫾ 14.6%; P ⫽ .049; post hoc study power, 71%). Meanwhile, the number of glaucoma medications after operation was not significantly different between the 2 groups (Figure 3). Visual acuity deteriorated in both groups during the 2-year follow-up and there were no significant betweengroup differences at any point during the study (Table 2; Figure 4). In postoperative month 24, the mean deviation of visual field results remained comparable with the preoperative value in those who successfully completed the trail in the Ahmed group. However, the Molteno group experienced worsened mean deviation of the visual field results in postoperative month 24 than before surgery (Table 2). 898 AMERICAN JOURNAL ● HYPERTENSIVE PHASE: A hypertensive phase was observed in 13 eyes (28.3%) after a mean of 5.5 ⫾ 1.7 weeks (median, 4 weeks, range, 1 to 11 weeks) in the Ahmed group. The mean IOP at the time of onset was 31.1 ⫾ 4.3 mm Hg, with an average number of antiglaucoma medications of 1.8 ⫾ 0.6. Of the 13 hypertensive eyes in the Ahmed valve group, resolution occurred in 4 eyes within OF OPHTHALMOLOGY JUNE 2010 10 months, and no other resolution occurred thereafter; treatment failed in 3 eyes, and in the remaining 6, IOP was controlled (⬍21 mm Hg with medications) at the follow-up visits, but did not meet the criteria for resolution. In the Molteno group, a hypertensive phase was observed in 8 eyes (17.4%) after a mean of 6 ⫾ 1.3 weeks (median, 5 weeks; range, 3 to 12 weeks). The mean IOP at the time of onset was 30.6 ⫾ 3.22 mm Hg, with an average number of antiglaucoma medications of 1.6 ⫾ 0.5. No resolution observed in the hypertensive eyes of the Molteno implant group: 2 failed and 6 continued using the same number of antiglaucoma medications without any improvement in IOP control. ● INTRAOPERATIVE AND POSTOPERATIVE COMPLICATIONS: There were no major intraoperative complica- tions. Postoperative complications were comparable in both groups (Table 3); there was no case of hypotony or devastating complications in both groups. 5-Fluorouracil was not applied for any patient after surgery. Bleb needling was performed in 10 (21.8%) and 9 (19. 6%) patients in the Ahmed and Molteno groups, respectively. No vision loss to no light perception was observed. DISCUSSION THIS RANDOMIZED CLINICAL TRIAL WAS DESIGNED TO IN- vestigate the success of the Ahmed valve compared with the Molteno implant in the surgical management of eyes with refractory glaucoma. ● INTRAOCULAR PRESSURE MEDICATIONS: After 2 years AND ANTIGLAUCOMA of follow-up, the level of IOP control was 49.7% and 41.9% in the Molteno and Ahmed groups, respectively. The Molteno group, compared with the Ahmed group, showed higher IOPs in postoperative day 1 and week 1. From postoperative month 1 until the end of the trial, IOP remained significantly lower in the Molteno group than in the Ahmed group. This is despite a comparable number of antiglaucoma medications between the 2 groups. The higher IOPs (Figure 2), mean number of antiglaucoma medications (Figure 3), and earlier administration of medications (Figure 3) within the first postoperative month in the Molteno group can be attributed to the temporary restriction of aqueous outflow by the absorbable ligature in the immediate postoperative period. The degree of IOP reduction after glaucoma drainage implant surgery may be dependent on capsular thickness and the total surface area of encapsulation. Lower postoperative IOP is expected with a thinner capsule and larger surface area of the drainage device. It has been reported that shunts with a larger surface area (e.g., the double-plate Molteno implant) may provide better IOP control,23,24 although early hypotony-related complications may be VOL. 149, NO. 6 AHMED VALVE VS more likely with these shunts. Nevertheless, there seems to be an upper limit to plate size beyond which other factors, such as the degree of encapsulation around the end plate, influence the final IOP. However, the ideal size of the end plate has not been identified precisely.25–32 ● VISUAL ACUITY AND VISUAL FIELD: Both groups showed approximately 1 Snellen line of deterioration in visual acuity, which is compatible with that reported in previous studies.9,10,12,33–35 This may be attributed to the progression of visual field defect, to the progression of lens opacity, which has been reported to be higher in glaucomatous eyes secondary to glaucoma surgery36 – 41 and antiglaucoma drug therapy,42– 44 or both. Whereas the final visual field score in the Ahmed group was not significantly different from the baseline value, the Molteno group had an approximately 1-dB loss in mean deviation score after 24 months, which was statistically significant (Table 2). Ironically, this happened despite lower mean postoperative IOPs achieved in the Molteno group than in the Ahmed group. We believe that this level of decrease in mean deviation in the Molteno group cannot be of clinical importance and may be attributed to decreasing visual acuity (Table 2) and increasing lens opacity (Table 3). Additionally, the Molteno group, compared with the Ahmed valve group, had poorer control of immediate postoperative IOPs, which may have resulted in deteriorated visual field results in the earlier postoperative period and resulted in poorer final visual field results despite better final general IOP control in the former group. Early postoperative IOP control may result in better visual field preservation, especially in those with severe glaucoma. Nevertheless, visual field assessment was not carried out during the first 3 postoperative months of the current study, and further studies are required to investigate this hypothesis. It seems that the achieved level of IOP control in both groups of this study was clinically sufficient to preserve visual field defect after 24 months. ● SURVIVAL ANALYSIS: Survival analysis did not show any significant difference between the 2 groups. The surgical success rate at the end point of this study was more than 80% in both groups. Surgical success rates for glaucoma drainage devices have been reported to be 22% to 100%.45 However, it is difficult to perform an accurate comparison between various studies because most clinical data were derived from retrospective studies with various demographic and surgical characteristics. Additionally, some results involving the Ahmed valves may not be valid for current practice because of the change from the polypropylene to the silicone Ahmed valves by many surgeons. The annual success rate decrement was 6% in the Ahmed group and 9% in the Molteno group, which seems to be less than the previously reported 10% to 15%.30,46 MOLTENO IMPLANT 899 ● HYPERTENSIVE PHASE: A hypertensive phase, as an early finding, has been reported after implantation of both the Molteno implant and Ahmed valve9,10,17,24,30,47; however, it is less common with nonvalved glaucoma drainage devices,17,31 mostly because of the widespread use of intraoperative tube ligation. The hypertensive phase was observed in 13 (28.3%) patients in the Ahmed group, which was less than previously reported rates of 84%,30 56%,17 and 50%.19 It is also less than that of our previous study (29.3%), where we used the same definition for hypertensive phase17 and reported the outcome of combined Ahmed valve drainage (model S2) and phacoemulsification.48 This may be because of the use of Ahmed valves with silicone material (FP7 model) in the current study. It has been shown previously that Ahmed valve tubes with polypropylene have a greater risk of encapsulation.17,20,21,30 Conversely, Mackenzie and associates reported a similar incidence of hypertensive phase in silicone and polypropylene material Ahmed valves.19 Although the Ahmed valve model FP7 has silicone material and a relatively larger (185 mm2) and more flexible end plate compared with the polypropylene model and the smaller (134 mm2) end plate of the Molteno implant, the incidence of a hypertensive phase was lower in the Molteno group compared with the Ahmed group (17.4% vs 28.3%). The explanation may lie in the immediate aqueous filtration that occurs with Ahmed valves and the delayed filtration with the ligated Molteno implants.11,31 Additionally, the rate may have been underestimated in our study because of the earlier administration of antiglaucoma medication in the Molteno group, compared with the Ahmed group. Resolution was observed in 4 of 13 patients and 0 of 8 patients in the Ahmed and Molteno groups, respectively. This supports the conclusions of Nouri-Mahdavi K and Capriole, who suggested that the so-called hypertensive phase is actually transient in a minority of the eyes and that most patients will need medication for at least the first postoperative year.17 They reported better IOP control and a significantly lower number of medications in the group without a hypertensive phase. However, Mackenzie and associates observed resolution of the hypertensive phase in most patients.19 This may be the result of the preference in that study for the application of bleb needling with 5-fluorouracil. Our preference in the management of the hypertensive phase was for administration of antiglaucoma medications rather than bleb needling. ate aqueous filtration through the Ahmed valve can stimulate a fibrotic response to inflammatory factors in the subconjunctival space, delayed flow with a ligated nonvalved implant may elicit a less fibrous reaction.11 Other factors, such as biomaterial characteristics, shape, and end plate consistency, which differ with different devices, have been linked to different rates of encapsulated blebs.20,21 In contrast to Wilson and associates, we reported all eyes with an encapsulated bleb regardless of whether the IOP was more or less than 21 mm Hg.12 This complication was managed initially by adding antiglaucoma medications and then by needling49 without an adjunctive antimetabolite. Bleb needling was performed in 10 patients in the Ahmed valve group and in 9 patients in the Molteno implant group. All cases with choroidal effusion and choroidal maculopathy responded to medical therapy with a corticosteroid. Those with conjunctival wound dehiscence were repaired with resuturing, and this was not considered a surgical failure. One patient with a flap anterior chamber in the Molteno group required reformation with viscoelastic. There were no ocular motility problems in either group. Hyphema was transient and inconsequential. Obstruction of the tube with fibrin was managed with corticosteroids. Cataract was responsible for loss of 2 Snellen lines or more in 6 (13%) and 8 (17.4%) phakic eyes in the Ahmed and Molteno groups, respectively. Gedde and associates reported higher rates of cataract progression (loss of ⱖ 2 Snellen lines) after 350-mm2 Baerveldt glaucoma implant administration (33%) and trabeculectomy (48%).36 With its relatively stringent inclusion and exclusion criteria, the study findings may not be applicable to all refractory glaucoma patients. Final analysis was performed on 59 study subjects, which is short of the 64 subjects that were deemed required by sample size estimation. However, the post hoc calculated power of the study was satisfactory, and the actual difference in mean IOP in postoperative month 24 between the 2 groups was more than the estimated figure of 1 mm Hg, which makes this shortfall less detrimental to the final conclusions. With the limited number of patients in this trial, we could not investigate accurately all the factors that may have influenced outcome and eventually can affect choice of glaucoma drainage implant before surgery. The trial data were analyzed according to the protocol, which potentially may affect the results and might have been a source of bias. In conclusion, this study corroborates previous findings regarding the success of both the Ahmed and Molteno groups in the surgical management of patients with refractory glaucoma. Both studied glaucoma drainage implants were comparable in survival analysis, surgical complications, and visual field stabilization. However, the Molteno group had better IOP control after the immediate postoperative period, and this device may be a better choice, especially in eyes with advanced glaucoma where more IOP reduction is required. ● INTRAOPERATIVE AND POSTOPERATIVE COMPLICATIONS: There were no intraoperative or devastating post- operative complications. All complications were transient and resolved spontaneously or with simple medical or surgical interventions; so, they were not considered to be surgical failures. The most common postoperative complication was an encapsulated bleb, which occurred more frequently with Ahmed valve implants. Whereas immedi900 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE 2010 THE AUTHORS INDICATE NO FINANCIAL SUPPORT OR FINANCIAL CONFLICT OF INTEREST. INVOLVED IN DESIGN OF STUDY (Nad.N., G.K., S.N., L.R, Nar.N.); Conduct of study (Nad.N., G.K., S.N., L.R., Nar.N.); Data collection (G.K., S.N., L.R.); Analysis and interpretation of data (M.R., B.M., Nar.N.); Preparation of the primary article or its critical revision (Nad.N., G.K., M.R., B.M., S.N., L..R, Nar.N.); Preparation of subsequent revisions (Nad.N., M.R., Nar.N.); and final approval of the article and its revisions (Nad.N., G.K., M.R., B.M., S.N., L..R, Nar.N.). The Ethics Committee of the Shaheed Beheshti University (M.C.), Tehran, Iran, and institutional review board at each clinical center (i.e., Imam Hossein Medical Center, Negah Eye Hospital, and Vanak Eye Surgery Center, Tehran, Iran) approved the study protocol. All patients provided informed consent in accordance with local regulations and the Declaration of Helsinki. The study is registered with ClinicalTrials.gov (registration no. NCT00971061). REFERENCES 1. The Fluorouracil Filtering Surgery Study Group. Five-year follow-up of the Fluorouracil Filtering Surgery Study. Am J Ophthalmol 1996;121:349 –366. 2. Broadway DC, Grierson I, Hitchings RA. Local effects of previous conjunctival incisional surgery and subsequent outcome of filtration surgery. Am J Ophthalmol 1998;125:805– 818. 3. Chen PP, Yamamoto T, Swada A, et al. Use of antifibrosis agents and glaucoma drainage devices in the American and Japanese Glaucoma Societies. J Glaucoma 1997;6:192–196. 4. Joshi AB, Parrish RK, Feuer WF. 2002 Survey of the American Glaucoma Society: practice preferences for glaucoma surgery and antifibrotic use. J Glaucoma 2005;14:172– 174. 5. Wilson RP, Cantor L, Katz LJ, et al. Aqueous shunts. Molteno versus Schocket. Ophthalmology 1992;99:672– 676; discussion 676 – 678. 6. Siegner SW, Netland PA, Urban RC Jr, et al. Clinical experience with Baerveldt glaucoma drainage implant. Ophthalmology 1995;102:1298 –1307. 7. Fellenbaum PS, Almeida AR, Minckler DS, Sidoti PA, Baerveldt G, Heuer DK. Krupin disk implantation for complicated glaucomas. Ophthalmology 1994;101:1178 –1182. 8. Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the Ahmed Glaucoma Valve Implant. Am J Ophthalmol 1995;120:23–31. 9. Ayyala RS, Zurakowski D, Smith JA, et al. A clinical study of the Ahmed glaucoma valve implant in advanced glaucoma. Ophthalmology 1998;105:1968 –1976. 10. Huang MC, Netland PA, Coleman AL, et al. Intermediateterm clinical experience with the Ahmed Glaucoma Valve implant. Am J Ophthalmol 1999;127:27–33. 11. Tsai JC, Johnson CC, Dietrich MS. The Ahmed shunt versus the Baerveldt shunt for refractory glaucoma: a single-surgeon comparison of outcome. Ophthalmology 2003;110:1814 – 1821. 12. Wilson MR, Mendis U, Smith SD, Paliwal A. Ahmed glaucoma valve implant vs trabeculectomy in the surgical treatment of glaucoma: a randomized clinical trial. Am J Ophthalmol 2000;130:267–273. 13. Anderson DR. Automated Static Perimetry. St. Louis: Mosby Year Book; 1992:84 – 85. 14. Heijl A, Bengtsson B. The effect of perimetric experience in patients with glaucoma. Arch Ophthalmol 1996;114:19 –22. 15. Kulze JC, Stewart WC, Sutherland SE. Factors associated with a learning effect in glaucoma patients using automated perimetry. Acta Ophthalmol 1990;68:681– 686. 16. Topouzis F, Coleman AL, Choplin N, et al. Follow-up of the original cohort with the Ahmed glaucoma valve implant. Am J Ophthalmol 1999;128:198 –204. VOL. 149, NO. 6 AHMED VALVE VS 17. Nouri-Mahdavi K, Capriole J. Evaluation of the hypertensive phase after insertion of the Ahmed glaucoma valve. Am J Ophthalmol 2003;136:1001–1008. 18. Ishida K, Netland PA, Costa VP, Shiroma L, Khan B, Ahmed II. Comparison of polypropylene and silicone Ahmed glaucoma valves. Ophthalmology 2006;113:1320 – 1326. 19. Mackenzie PJ, Schertzer RM, Isbister CM. Comparison of silicone and polypropylene Ahmed glaucoma valves: twoyear follow-up. Can J Ophthalmol 2007;42:227–232. 20. Ayyala RS, Harman LE, Michelini-Norris B, et al. Comparison of different biomaterials for glaucoma drainage devices: part 1. Arch Ophthalmol 1999;117:233–236. 21. Ayyala RS, Michelini-Norris B, Flores A, Hallar E, Margo CE. Comparison of different biomaterials for glaucoma drainage devices: part 2. Arch Ophthalmol 2000;118: 1081–1084. 22. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 2007;39:175–191. 23. Taglia DP, Perkins TW, Gangnon R, et al. Comparison of the Ahmed glaucoma valve, the Krupin eye valve with disk, and the double-plate Molteno implant. J Glaucoma 2002;11: 347–353. 24. Heuer DK, Lloyd MA, Abrams DA, et al. Which is better? One or two? A randomized clinical trial of single-plate versus double-plate Molteno implantation for glaucoma in aphakia and pseudophakia. Ophthalmology 1992;99:1512–1519. 25. Lloyd MA, Baeverdlt G, Felenbaum PS, et al. Intermediateterm results of a randomized clinical trial of the 350- versus the 500-mm2 Baerveldt implant. Ophthalmology 1994;101: 1456 –1463. 26. Smith MF, Doyle JW, Sherwood MB. Comparison of the Baerveldt glaucoma implant with the double-plate Molteno drainage implant. Arch Ophthalmol 1995;113:444 – 447. 27. Britt MT, LaBree LD, Lloyd MA, et al. Randomized clinical trial of the 350-mm2 versus 500-mm2 Baerveldt implant: longer term results: is bigger better? Ophthalmology 1999; 106:2312–2318. 28. Tsai JC, Johnson CC, Kammer JA, Dietrich MS. The Ahmed shunt versus the Baerveldt shunt for refractory glaucoma II: longer-term outcomes from a single surgeon. Ophthalmology 2006;113:913–917. 29. Broadway DC, Iester M, Schulzer M, Douglas GR. Survival analysis for success of Molteno tube implants. Br J Ophthalmol 2001;85:689 – 695. 30. Ayyala RS, Zurakowski D, Monshizadeh R, et al. Comparison of double-plate Molteno and Ahmed glaucoma valve in patients with advanced uncontrolled glaucoma. Ophthalmic Surg Lasers 2002;33:94 –101. MOLTENO IMPLANT 901 31. Hong CH, Arosemena A, Zurakowski D, Ayyala RS. Glaucoma drainage devices: a systematic literature review and current controversies. Surv Ophthalmol 2005;50:48 – 60. 32. Goulet RJ 3rd, Phan AD, Cantor LB, WuDunn D. Efficacy of the Ahmed S2 glaucoma valve compared with the Baerveldt 250-mm2 glaucoma implant. Ophthalmology. 2008;115:1141– 1147. 33. Das JC, Chaudhuri Z, Sharma P, Bhomaj S. The Ahmed glaucoma valve in refractory glaucoma: experiences in Indian eyes. Eye 2005;19:183–190. 34. Wilson MR, Mendis U, Paliwal A, Haynatzka V. Long-term follow-up of primary glaucoma surgery with Ahmed glaucoma valve implant versus trabeculectomy. Am J Ophthalmol 2003;136:464 – 470. 35. Ishida K, Netland PA. Ahmed glaucoma valve implantation in African American and white patients. Arch Ophthalmol 2006;124:800 – 806. 36. Gedde SJ, Herndon LW, Brandt JD, et al. Surgical complications in the Tube versus Trabeculectomy Study during the first year of follow-up. Am J Ophthalmology 2007;143:23–31. 37. Hylton C, Congdon N, Friedman D, et al. Cataract after filtration surgery. Am J Ophthalmol 2003;135:231–232. 38. AGIS (Advanced Glaucoma Intervention Study) Investigators. The Advanced Glaucoma Intervention Study: 8. Risk of cataract formation after trabeculectomy. Arch Ophthalmol 2001;119:1771–1779. 39. Lichter PR, Musch DC, Gillespie BW, et al. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001;108:1943–1953. 40. Collaborative Normal-Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with ther- 902 AMERICAN JOURNAL 41. 42. 43. 44. 45. 46. 47. 48. 49. OF apeutically reduced intraocular pressures. Am J Ophthalmol 1998;126:487– 497. The AGIS Investigators. The advanced glaucoma intervention study (AGIS), 6: effect of cataract on visual field and visual acuity. Arch Ophthalmol 2000;118:1639 –1652. Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol 2002;120:701–713. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol 2002; 120:1268 –1279. Leske MC, Wu SY, Nemesure B, et al. Risk factors for incident nuclear opacities. Ophthalmology 2002;109:1303– 1308. Schwartz KS, Lee RK, Gedde SJ. Glaucoma drainage implants: a critical comparison of types. Curr Opin Ophthalmol 2006;17:181–189. Mills RP, Reynolds A, Emond MJ, et al. Long-term survival of Molteno glaucoma drainage devices. Ophthalmology 1996;103:299 –305. Molteno TE, Dempster AG. Methods of controlling bleb fibrosis around drainage implants. In: Mills KB, ed. Fourth International Symposium of the Northern Eye Institute. Manchester, UK: Pergamon Press; 1988:192–211. Nassiri N, Nassiri N, Sadeghi Yarandi S, et al. Combined phacoemulsification and Ahmed valve glaucoma drainage implant: a retrospective case series. Eur J Ophthalmol 2008; 18:291–298. Lam DSC, Lai JSM, Chua JKH, et al. Needling revision of glaucoma drainage device filtering blebs. Ophthalmology 1998;105:1127. OPHTHALMOLOGY JUNE 2010