Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
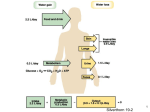
Polyuria -Polyuria defined as >3L/day -CAUTION! Polyuria not necessarily increased frequency (increased frequency with small volumes each time can lead to normal overall urine volume production). -2 major causes of polyuria: (a) water diuresis (b) solute (osmotic) diuresis -If polyuria present (>3L/day), can differentiate water from solute diuresis by urine osmolality: water diuresis urine osmolality <250 mosmol/L solute diuresis urine osmolality >300 mosmol/L -Causes of solute diuresis (all due to reduced absorption of NaCl and water in proximal tubule): (a) glucose (poorly controlled diabetes mellitus: most common cause of solute diuresis) (b) mannitol (usually iatrogenic) (c) urea (e.g. from high protein feeding both enterally and parenterally) (d) radiocontrast media -Causes of water diuresis: -2 main classifications: (a) primary polydipsia (b) Diabetes insipidus (both central and nephrogenic) -usually polyuria, excessive thirst (due to hypotonic urine excretion), and polydipsia. (a) primary polydipsia: increased water intake, thereby leading to polyuria Causes: -psychogenic, medications, hypothalamic diseases. (b) diabetes insipidus: (i) central (low secretion of ADH) (ii) nephrogenic (ADH-resistant kidney) (i) Causes of central DI : -idiopathic (can be autosomal dominant or spontaneous) -post-hypophysectomy (therefore decreased ADH) -CNS neoplasms -trauma -CNS aneurysm compression -CNS infection (ii) Causes of nephrogenic: -Congenital -Pyelonephritis -Hypercalcemia -Hypokalemia (reversible causes) -Drugs/toxins (ex. lithium) -Analgesic nephropathy -Renal Amyloidosis -Can differentiate by (a) Plasma ADH level: -low in central diabetes insipidus -high in nephrogenic diabetes insipidus (b) Water deprivation test -Best method for making distinction Water deprivation test A. B. C. D. II. Fluid restrict patient before test and follow up the serum osmolality. Follow serum osmolality to steady state 1. serum osmolality should approach 295 mOsm/L 2. measure serum osmolality hourly until endpoint: Two values are within 30 mOsm/kg of each other or weight loss exceeds 3-5%. Administer of ADH 1. Vasopressin 5 units SC or 2. Intranasal ddAVP 10 ug Measure Serum Osmolality 1 hour after ADH administered Interpretation A. Water deprivation effect on urine concentrating ability 1. No response in Nephrogenic DI 2. No response in Central DI B. Exogenous ADH effect on urine concentrating ability 1. Corrects Central DI 2. Does not correct Nephrogenic DI Water Diuresis Appropriate Inappropriate Primary Polydipisia Central DI (Uosm <250mosm/L) Nephrogenic DI Solute Diuresis Post-obstructive diuressi Hyperglycemia (Uosm >300mosm/L) Saling Loading High-protein diet Salt Wasting Nephropathy