Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Issues in Emerging Health Technologies
Issue 36
August 2002
Uterine Artery Embolization for the
Treatment of Fibroids
Summary
9 Uterine artery embolization (UAE), or
uterine fibroid embolization, is a nonsurgical treatment for uterine fibroids
that preserves the uterus and offers
women an alternative to surgical
procedures such as hysterectomy and
myomectomy.
9 Evidence from controlled trials comparing
fibroid treatments is not yet available.
Case series reports indicate that UAE is a
relatively safe and effective treatment for
symptomatic fibroids.
materials are injected until the blood flow to the
fibroid ceases.2 Patients are usually hospitalized
overnight, mainly for pain management, but the
hospital stay is generally less than 24 hours.3
Smaller and submucosal fibroids appear more
likely to be reduced in volume after UAE than
other types of fibroids.4
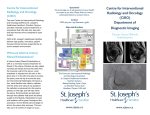
Figure 1.
Uterine Fibroid Embolization
uterine artery
9 The effect of UAE on fertility and pregnancy is not known, though pregnancies
following UAE have been reported.
The Technology
Uterine fibroids are benign growths in the walls
of the uterus. Most fibroids do not require treatment, but some women experience abnormal
bleeding causing anemia, pain and pelvic pressure caused by an enlarged uterus. Fibroids may
sometimes cause infertility.1
Uterine artery embolization (UAE) closes the
blood supply to the uterine arteries, causing death
of the tissue and shrinkage of the fibroids. In
UAE the patient is sedated and given only local
anesthesia. The procedure is performed by an
interventional radiologist. A catheter is inserted
through a small incision in the groin and threaded
through the femoral artery to the uterine arteries
(Figure 1). Under fluoroscopic guidance, embolic
fibroid
catheter
Infographic by Renée Gordon
9 UAE may reduce health care costs associated with treating fibroids through
shorter hospital stays and faster
recoveries.
uterus
polyvinyl particles
femoral artery
Reprinted with permission: FDA Consumer Magazine5
Regulatory Status
UAE is a medical procedure and, as such, is not
licensed by Health Canada. The embolization
materials used include polyvinyl alcohol foam
particles (PVA), tris-acryl gelatin microspheres,
absorbable gelatin sponges and coils. These
devices have been licensed in Canada and elsewhere for general embolization purposes, but not
specifically for UAE. The superiority of any particular embolization device has not yet been
demonstrated.6
Two companies have filed applications with the
US Food and Drug Administration (FDA) for
approval of embolization agents for UAE:
BioSphere for two types of tris-acryl gelatin
microspheres (Embosphere® and EmboGold™
Microspheres), and Boston Scientific for Contour
PVA®.
The Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
is a non-profit organization funded by the federal, provincial and territorial governments. (www.ccohta.ca)
Patient Group
Thirty to forty per cent of women over the age of
30 may have uterine fibroids, and the incidence is
higher in African-American women.7 Most
fibroids are asymptomatic and only a minority
require treatment.8 Nevertheless, fibroids were
the main reason for about 40% of the 49,000 hysterectomies performed in Canadian women over
the age of 35 in 1996-1997.9 In 1999-2000, 3,000
Canadian women underwent myomectomy (surgical removal of fibroids from the uterus).10
Current Practice
Drug therapy with gonadotropin-releasing hormone (GnRH) analogs may be used to shrink
fibroids by blocking the natural production of
estrogen. GnRH analogs are used for short
periods of time, mainly to decrease the size of
fibroids prior to surgery, or when surgery is not
an option.5,11 Side effects of the drugs, such as
menopausal symptoms and loss of bone density,
limit their long-term use. Fibroids often recur
when drug therapy is discontinued. These drugs
are expensive and may not be covered by provincial health insurance plans (Gaylene Pron,
University of Toronto, Toronto: personal communication, 2002 June 10).
Hysterectomy is the standard treatment for symptomatic fibroids in women who have completed
child bearing.12 Abdominal hysterectomy is the
most common type, though vaginal hysterectomies now account for about a third of all hysterectomies in Canada.11 These procedures are
sometimes performed laparoscopically. Reports
of major and minor complications associated
with hysterectomy range widely, from 0.5 to
43%.11 The average length of hospitalization for
abdominal hysterectomy in Canada is about four
days.11
Myomectomy may be an alternative treatment for
women who want to preserve their fertility.13
Laparoscopic myomectomy offers a shorter
recovery time than open abdominal myomecto-
my, but it is not suitable for all types of fibroids.
General anesthesia is required14 and adhesions,
hemorrhage and infection may occur. The procedure is associated with a 5% rate of complications.15 Canadian data indicate an average
hospital stay of 3.6 days for myomectomy.10
Fibroids often recur following myomectomy and
may require further treatment.11
Administration and Cost
Information on the cost of UAE in Canada has
not been published. One Ontario hospital estimated the following charges for UAE: pre-admission
testing ($400), ultrasound ($240), overnight
surgical ward stay ($3,700), technical fees and
materials ($1,300), anesthetist and morphine pain
pump ($1,040). The main difference from other
treatments is in the length of stay - one day for
UAE compared to three or four days for
myomectomy or hysterectomy (Gaylene Pron,
2002 April 24). A recent study at McGill
University compared in-patient hospital costs of
abdominal myomectomy, total abdominal hysterectomy, vaginal hysterectomy and UAE in 545
women treated for fibroids.16 UAE had the shortest hospital stay and the lowest in-patient nursing
costs (an average cost of $1,007 for UAE, compared to $1,781 for myomectomy and $1,933 for
total abdominal hysterectomy).
Rate of Technology Diffusion
UAE has been widely publicized in the popular
media and there is considerable demand for this
procedure. As many as 20,000 to 25,000 women
have been treated with UAE worldwide since it
was first introduced about 10 years ago.17
The Society of Interventional Radiology web
site18 lists over 20 Canadian physicians who perform UAE. Most Canadian teaching hospitals,
and some community hospitals now have interventional radiologists on staff. However, many
interventional radiologists do not have hospital
admitting privileges (Gaylene Pron, 2002 June
10).
The Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
is a non-profit organization funded by the federal, provincial and territorial governments. (www.ccohta.ca)
Concurrent Developments
Myolysis is a laparoscopic surgical technique that
uses electrical or laser coagulation to destroy the
fibroid or its blood supply. This is performed following several months of GnRH analog therapy
to shrink the fibroid. The procedure leaves the
uterus intact, but it may cause adhesions.19
Cryomyolysis involves "freezing" the fibroids.
Published evidence on the long-term effectiveness of this treatment is lacking.12
Mifepristone (RU-486) is a synthetic steroid that
may effectively treat fibroids, without adverse
effects on bone density.20 Mifepristone, commonly
known as the "abortion pill", is not yet available
in Canada.
Laparoscopic bipolar coagulation ("surgical
embolization" of the uterine arteries)21 using general anesthesia has been reported. Clinical results
were similar to those reported in UAE case
series, for example, ultrasound measures of
reductions in uterine volume (46%) and dominant
fibroid volume (76%). Results from long-term
follow-up are not yet available.
Other treatments under investigation for fibroids
include the use of high-intensity focused ultrasound, laser, or radiofrequency ablation, and a
'combination procedure' that uses UAE to shrink
fibroids followed by myomectomy to remove
remaining fibroids.22,23
will be published this year (Gaylene Pron, 2002
February 20). Preliminary results reported 50%
shrinkage of fibroids after UAE at three months
follow-up and continued shrinkage for up to one
year. Menorrhagia improved in about 80% of the
women in the trial.35
The submissions for regulatory approval of
embolization agents for UAE to the FDA were
based on two US trials: one trial that compared
women who had UAE to a cohort of women who
had hysterectomies, and another trial based on a
comparison with women who had myomectomies.36,37In addition to the US trials, a randomized controlled trial of 200 women, comparing
UAE to hysterectomy and myomectomy, is
underway in Scotland, but results are not
expected for two years.13
The Cardiovascular and Interventional Radiology
Research and Education Foundation (CIRREF) in
the US has created a Uterine Artery Embolization
(UAE) Fibroid Registry for Outcomes Data
(FIBROID). Its purpose is to refine UAE methods and to collect data on the safety and longterm effectiveness of UAE, and its impact on
patients' quality of life and fertility. Over 2,000
patients have been enrolled in the registry, but
analyses of the data are not yet available.38
Adverse Effects
To date, the published evidence on UAE is from
case series.24-34 Results from these series seem
similar: heavy bleeding and uterine bulk are controlled in 85-90% of patients.28 About 80% of
women reported a return to normal activities
within four days of UAE, (90% within ten
days).14
The mortality rate for UAE has been estimated as
between 0.02%-0.1%39,40 while that for hysterectomy is estimated at 0.6%.41 UAE is associated
with complications such as vaginal discharge,
allergic reactions to the contrast media and
hematoma formations at the puncture site.8
Postembolization syndrome (fever, nausea, vomiting, leukocytosis and flu-like symptoms lasting
for several days) is common. This condition is
self-limiting but can be difficult to distinguish
from infection.2
The first phase of a Canadian prospective,
multi-centre trial of 555 women was recently
completed. The trial examined the safety, patient
acceptability, and efficacy of UAE. The results
Most patients experience moderate to severe pain
following UAE and require pain control, antiinflammatory and sometimes anti-nausea medications for several days. Patient-controlled
The Evidence
The Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
is a non-profit organization funded by the federal, provincial and territorial governments. (www.ccohta.ca)
analgesia is commonly recommended.
Ovarian failure (premature menopause), perhaps
due to non-targeted embolization of the arteries
supplying the ovaries, has been reported at rates
from 1-15%.13,35,42,43 Other risks include thrombosis,44 radiation exposure45,46 and failure to detect a
rare type of uterine carcinoma, leiomyosarcoma,
using the standard pre-operative tests.27 The effect
of UAE on fertility is unknown, though pregnancies following UAE have been reported in
several studies.47,48
Complications from UAE may require some
women to have a subsequent hysterectomy. Eight
of over 500 patients in the Canadian trial of UAE
required a hysterectomy due to complications.35
Other studies have reported a risk from 0.7 to
10%.49
Implementation Issues
Until recently gynecologists treated uterine
fibroids, but interventional radiologists perform
UAE. Pre-operative testing and post-operative
care require a multidisciplinary approach and the
expertise of both specialties.
The techniques used for UAE vary between centres and physicians.6 The optimum level of
embolization and the most effective embolization
materials have not yet been determined.37
The case series published thus far show similar
results, though uncontrolled trials such as case
series tend to overestimate the efficacy of new
treatments.50 Investi-gators from the Canadian
trial are seeking funding for long-term follow-up
of participants. The results of such studies may
clarify uncertainties surrounding the long-term
effectiveness of UAE and its effect on fertility.
Some researchers believe UAE should continue
to be monitored, either through trials or national
registries, until these areas of uncertainty have
been resolved.51,52
There is a high rate of patient satisfaction with
UAE. Women's perceptions are that UAE offers a
permanent treatment for fibroids, preserving the
uterus and avoiding major surgery and prolonged
convalescence.53 The reduced hospital stay for
UAE compared with hysterectomy and myomectomy, and a quicker recovery and return to work,
may reduce the health care and societal costs
associated with this condition.
References
1.
Haney AF. Clinical decision making regarding
leiomyomata: what we need in the next millenium.
Environ Health Perspect 2000;108 Suppl 5:835-9.
2. Goodwin SC, Wong GC. Uterine artery embolization for uterine fibroids: a radiologist's perspective.
Clin Obstet Gynecol 2001;44(2):412-24.
3. Patient's guide: uterine artery embolization at
Georgetown University. In: Uterine artery
embolization [database online]. Washington, DC:
Georgetown University Hospital. Division of
Vascular and Interventional Radiology; 2002.
Available: http://www.fibroidoptions.com/
ptguide.htm (accessed 2002 Feb 7).
4. Spies JB, Roth AR, Jha RC, Gomez-Jorge J, Levy
EB, Chang TC, et al. Leiomyomata treated with
uterine artery embolization: factors associated with
successful symptom and imaging outcome.
Radiology 2002;222(1):45-52.
5. Bren L. Alternatives to hysterectomy. New technologies, more options. FDA Consum
2001;35(6):23-8.
6. Brody DP. Uterine fibroid embolization: practice
considerations. Cardiovascular Radiology
Newsletter [serial online] 1999:3-7. Available:
http://www.americanheart.org/downloadable/heart/3
422_CVRf99.pdf (accessed 2002 May 8).
7. Medical encyclopedia:uterine fibroids. In:
MEDLINEplus [database online]. Bethesda, MD:
U.S. National Library of Medicine; 2001. Available:
http://www.nlm.nih.gov/medlineplus/ency/article/000914.htm (accessed 2002 May 8).
8. Andersen PE, Lund N, Justesen P, Munk T, Elle B,
Floridon C. Uterine artery embolization of symptomatic uterine fibroids. Initial success and shortterm results. Acta Radiol 2001;42(2):234-8.
9. Millar WJ. Hysterectomy, 1981/82 to 1996/97.
Health Reports 2001;12(2):9-22.
10. Myomectomy data: CCP Code: 80.19; 1999/2000.
Toronto, ON: Canadian Institute for Health
Information; 2002.
11. Lefebvre G, Allaire C, Jeffrey J, Vilos G. SOGC
clinical practice guidelines: hysterectomy. J Obstet
Gynaecol Can 2002;24(1):37-48. Available:
http://sogc.medical.org/SOGCnet/sogc_docs/
common/guide/pdfs/ps109.pdf (accessed 2002
Apr 22).
The Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
is a non-profit organization funded by the federal, provincial and territorial governments. (www.ccohta.ca)
12. Olive DL. Review of the evidence for treatment of
leiomyomata. Environ Health Perspect 2000;108
Suppl 5:841-3.
13. Lumsden MA. Embolization versus myomectomy
versus hysterectomy: which is best, when? Hum
Reprod 2002;17(2):253-9.
14. Smith SJ. Uterine fibroid embolization. Am Fam
Physician 2000;61(12):3601-2.
15. Embolization found more effective than surgery for
uterine fibroids. Health Technol Trends
2001;13(5):5-6,8.
16. Tulandi T. Cost analysis of myomectomy, hysterectomy and uterine artery embolization [abstract].
11th World Congress on Human Reproduction;
2002 Jun 1; Montreal, PQ: McGill University; 2002.
17. Uterine artery embolization procedure. In: Uterine
artery embolization [database online].
[Washington, DC]: Georgetown University Hospital.
Division of Vascular and Interventional Radiology;
2002. Available: http://www.fibroidoptions.com/
embol.htm (accessed 2002 Feb 7).
18. Find an IR who performs UFE. In: Society of
Interventional Radiology [database online].
Fairfax (VA): SIR; 2002. Available:
http://directory.scvir.org/eseries/scriptcontent/index_
members_search.cfm?section=customer (accessed
2002 Jul 31).
19. Olive DL. New approaches to the management of
fibroids. Obstet Gynecol Clin North Am
2000;27(3):669-75.
20. Guidelines for the management of uterine fibroids:
summary of recommendations. In: Guideline
library [database online]. Wellington, NZ: New
Zealand Guidelines Group; 2000. Available:
http://www.nzgg.org.nz/library/gl_complete/
gynae_uterinefibroids/summary.cfm (accessed
2002 Apr 17).
21. Liu WM, Ng HT, Wu YC, Yen YK, Yuan CC.
Laparoscopic bipolar coagulation of uterine vessels:
a new method for treating symptomatic fibroids.
Fertil Steril 2001;75(2):417-22.
22. Health technology forecast. Plymouth Meeting,
PA: ECRI; 2002.
23. Stenson J. Radiofrequency ablation shows promise
as fibroid treatment. Reuters Health [serial online]
2002 May 8. Available:
http://www.asco.org/Reuters/May02/050802/050802
Radiofrequency.htm (accessed 2002 Jun 24).
24. Spies JB, Ascher SA, Roth AR, Kim J, Levy EB,
Gomez-Jorge J. Uterine artery embolization for
leiomyomata. Obstet Gynecol 2001;98(1):29-34.
25. Hutchins FL, Jr., Worthington-Kirsch R, Berkowitz
RP. Selective uterine artery embolization as primary
treatment for symptomatic leiomyomata uteri. J Am
Assoc Gynecol Laparosc 1999;6(3):279-84.
26. Ravina JH, Aymard A, Ciraru-Vigneron N, Ledreff
O, Merland JJ. [Arterial embolization of uterine
myoma: results apropos of 286 cases]. J Gynecol
Obstet Biol Reprod (Paris) 2000;29(3):272-5.
27. McLucas B, Adler L, Perrella R. Uterine fibroid
embolization: nonsurgical treatment for symptomatic fibroids. J Am Coll Surg 2001;192(1):95-105.
28. Spies JB. Physician's resource: literature review. In:
Uterine artery embolization [database online].
Washington, DC: Georgetown University Medical
Center; 2001. Available: http://www.fibroidoptions.
com/pr-lit.htm (accessed 2001 Oct 31).
29. Goodwin SC, McLucas B, Lee M, Chen G, Perrella
R, Vedantham S, et al. Uterine artery embolization
for the treatment of uterine leiomyomata midterm
results. J Vasc Interv Radiol 1999;10(9):1159-65.
30. Siskin GP, Stainken BF, Dowling K, Meo P, Ahn J,
Dolen EG. Outpatient uterine artery embolization
for symptomatic uterine fibroids: experience in 49
patients. J Vasc Interv Radiol 2000;11(3):305-11.
31. Worthington-Kirsch RL, Popky GL, Hutchins FL, Jr.
Uterine arterial embolization for the management of
leiomyomas: quality-of-life assessment and clinical
response. Radiology 1998;208(3):625-9.
32. Pelage JP, Le Dref O, Soyer P, Kardache M, Dahan
H, Abitbol M, et al. Fibroid-related menorrhagia:
treatment with superselective embolization of the
uterine arteries and midterm follow-up. Radiology
2000;215(2):428-31.
33. Bradley EA, Reidy JF, Forman RG, Jarosz J, Braude
PR. Transcatheter uterine artery embolisation to
treat large uterine fibroids. Br J Obstet Gynaecol
1998;105(2):235-40.
34. Brunereau L, Herbreteau D, Gallas S, Cottier JP,
Lebrun JL, Tranquart F, et al. Uterine artery
embolization in the primary treatment of uterine
leiomyomas: technical features and prospective follow-up with clinical and sonographic examinations
in 58 patients. AJR Am J Roentgenol
2000;175(5):1267-72.
35. Jenkins K. Fibroid treatment gives women options.
Healthy Woman 2002;2(2):22-4.
36. Spies JB, Benenati JF, Worthington-Kirsch RL,
Pelage JP. Initial experience with use of tris-acryl
gelatin microspheres for uterine artery embolization
for leiomyomata. J Vasc Interv Radiol
2001;12(9):1059-63.
37. Embolic agents: choice of particles for uterine artery
embolization for leiomyomata. In: Uterine Artery
Embolization [database online]. [Washington, DC]:
Georgetown University Hospital. Division of
Vascular and Interventional Radiology; 2002.
Available: http://www.fibroidoptions.com/
agents.htm (accessed 2002 Feb 7).
The Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
is a non-profit organization funded by the federal, provincial and territorial governments. (www.ccohta.ca)
38. Cardiovascular and Interventional Radiology
Research and Education Fund, Society of
Interventional Radiology. Registry Progress. In:
UAE FIBROID Registry [database online].
Fairfax (VA): CIRREF; 2002. Available:
http://www.fibroidregistry.org/results/Jul02/
results.htm (accessed 2002 Jul 2).
39. Dover RW, Torode HW, Briggs GM. Uterine artery
embolisation for symptomatic fibroids. Med J
Aust 2000;172(5):233-6.
40. Uterine fibroid embolization for the treatment of
fibroids. [Windows on medical technology].
Plymouth Meeting (PA): ECRI Health Technology
Assessment Information Service; 2001.
41. Simon JR, Silverstein MI. Uterine artery embolization for fibroids: procedure, results, and complications. Applied Radiology 2001;30(7 Suppl):17-28.
42. Chrisman HB, Saker MB, Ryu RK, Nemcek AA,
Jr., Gerbie MV, Milad MP, et al. The impact of
uterine fibroid embolization on resumption of
menses and ovarian function. J Vasc Interv Radiol
2000;11(6):699-703.
43. Ryu RK, Chrisman HB, Omary RA, Miljkovic S,
Nemcek AA, Jr., Saker MB, et al. The vascular
impact of uterine artery embolization: prospective
sonographic assessment of ovarian arterial circulation. J Vasc Interv Radiol 2001;12(9):1071-4.
44. Centre for Devices and Radiological Health (U.S.).
Obstetrics and Gynecology Devices Panel SixtyFourth Meeting. Rockville, MD: U.S. Dept. of
Health and Human Services, Public Health Service,
Food and Drug Administration, Center for Devices
and Radiological Health; 2001. Available:
http://www.fda.gov/ohrms/dockets/ac/01/
transcripts/3753t2.pdf (accessed 2002 Mar 7).
45. Nikolic B, Spies JB, Lundsten MJ, Abbara S.
Patient radiation dose associated with uterine artery
embolization. Radiology 2000;214(1):121-5.
46. Nikolic B, Spies JB, Campbell L, Walsh SM,
Abbara S, Lundsten MJ. Uterine artery embolization: reduced radiation with refined technique. J
Vasc Interv Radiol 2001;12(1):39-44.
47. McLucas B, Goodwin S, Adler L, Rappaport A,
Reed R, Perrella R. Pregnancy following uterine
fibroid embolization. Int J Gynaecol Obstet
2001;74(1):1-7.
48. Ravina JH, Vigneron NC, Aymard A, Le Dref O,
Merland JJ. Pregnancy after embolization of uterine myoma: report of 12 cases. Fertil Steril
2000;73(6):1241-3.
49. Goodwin SC, Bonilla SM, Sacks D, Reed RA,
Spies JB, Landow WJ, et al. Reporting standards
for uterine artery embolization for the treatment of
uterine leiomyomata. J Vasc Interv Radiol
2001;12(9):1011-20.
50. Hurst BS, Stackhouse DJ, Matthews ML,
Marshburn PB. Uterine artery embolization for
symptomatic uterine myomas. Fertil Steril
2000;74(5):855-69.
51. Braude P, Reidy J, Nott V, Taylor A, Forman R.
Embolization of uterine leiomyomata: current concepts in management. Hum Reprod Update
2000;6(6):603-8.
52. Broder MS, Landow WJ, Goodwin SC, Brook RH,
Sherbourne CD, Harris K. An agenda for research
into uterine artery embolization: results of an
expert panel conference. J Vasc Interv Radiol
2000;11(4):509-15.
53. Nevadunsky NS, Bachmann GA, Nosher J, Yu T.
Women's decision-making determinants in choosing uterine artery embolization for symptomatic
fibroids. J Reprod Med 2001;46(10):870-4.
This brief was prepared by Leigh-Ann Topfer, MLS
and David Hailey, PhD
and has been peer reviewed by:
Dr. Bernhard Gibis
National Association of Statutory Health
Insurance Physicians
Berlin, Germany
Dr. Jeff Barkun
Department of Surgery, Royal Victoria Hospital
Montreal, Quebec
Dr. Gaylene Pron
Epidemiologist, Department of Public Health Sciences,
University of Toronto
Toronto, Ontario
ISSN 1488-6324 (online)
ISSN 1488-6316 (print)
Publications Agreement Number 40026386
The Canadian Coordinating Office for Health Technology Assessment (CCOHTA)
is a non-profit organization funded by the federal, provincial and territorial governments. (www.ccohta.ca)